Original Article - DOI:10.33594/000000760
Accepted 22 February 2025 - Published online 28 February 2025
Effective Treatment of Cartilage Abnormalities in Middle-Aged Individuals (Aged 45-60): Bounding Molecular Biology with Microfracture and Hyalofast Membrane Approach Show Positive Outcomes
bWolf Project Studio Krzysztof Król, ul. Gdańska 79/D01, 90-613 Łódź,
cAECC University College, Bournemouth, UK
Keywords
Abstract
Background/Aims:
In recent years, significant progress has been made in treating cartilage lesions, leading to various techniques aimed at articular surface regeneration. However, the impact of patient age on treatment outcomes remains understudied, despite its recognized influence on effectiveness. Many studies impose upper age limits, resulting in limited data on middle-aged patients, a group frequently undergoing cartilage repair. Age-related physiological changes, including a decline in regenerative capacity and alterations in proteoglycan composition, are believed to affect treatment success. This study investigates the clinical outcomes of cartilage repair in patients aged 45 to 60, specifically evaluating the effectiveness of microfracture combined with Hyalofast membrane implantation.Methods:
Patients aged 45–60 undergoing microfracture with Hyalofast membrane implantation were evaluated. Short- and medium-term outcomes were assessed using the KOOS and SF-36 questionnaires preoperatively and at 6- and 12-month follow-ups. Functional evaluations and MRI analyses were conducted by expert reviewers. Additionally, an intensive rehabilitation program was initiated immediately post-surgery. Statistical analysis was performed using a one-way repeated-measures ANOVA to compare preoperative, 6-month, and 12-month results, with Tukey’s post-hoc test applied for multiple comparisons. Clinical significance was assessed using Cohen’s d effect size, with standard thresholds for small, medium, and large effects.Results:
The combined microfracture and Hyalofast membrane approach, along with early rehabilitation, yielded promising results. Key benefits included reduced inflammation, improved membrane integration, and decreased subchondral edema.Conclusion:
These findings support the feasibility of this treatment strategy, highlighting its potential to enhance joint function, alleviate pain, and improve the overall quality of life in middle-aged patients.Introduction
Focal cartilage abnormalities in the knee can cause significant pain and disability [1, 2], and can affect quality of life to the same level as osteoarthritis (OA) [3]. Because articular cartilage has limited regeneration capacity, cartilage abnormalities frequently develop to OA [1]. Cartilage abnormalities have thus been identified as a key predictor of total knee arthroplasty (TKA) in patients over the age of 45 [4] and therefore the objective of cartilage repair in middle age is to delay or eliminate the necessity for TKA.
Cartilage aging involves complex molecular processes that gradually impair its structure and function, reducing its resilience to mechanical stress and increasing susceptibility to degeneration, including osteoarthritis [5]. These molecular changes affect the extracellular matrix (ECM), cellular functions, signaling pathways, and interactions between cartilage and surrounding structures (Fig. 1) [6]. Understanding these mechanisms is essential for developing therapies to slow cartilage degradation. Proteoglycans, particularly aggrecan, are vital macromolecules within the cartilage ECM that provide compressive strength and facilitate water retention, essential for cartilage resilience [7]. Aggrecan consists of a core protein linked to numerous glycosaminoglycan (GAG) chains, such as chondroitin sulfate and keratan sulfate [8]. These highly sulfated, negatively charged GAG chains attract cations and water molecules through osmotic pressure, enabling the tissue to withstand compressive forces [9]. With aging, chondrocytes produce less aggrecan, and GAG chain structures change, reducing their ability to retain water [10, 11]. Enzymes like chondroitinases degrade chondroitin sulfate chains more rapidly in aged cartilage, further compromising the matrix structure [12]. Hyaluronic acid (HA), a large non-sulfated GAG synthesized by hyaluronan synthases (HAS1, HAS2, HAS3), act as a backbone for proteoglycan aggregates [9]. Aging reduces HAS enzymes expression, lowering HA synthesis [13], while increased hyaluronidases activity fragments HA chains [14]. These shorter HA fragments form weaker aggregates with aggrecan, destabilizing the ECM and increasing its permeability, leading to essential ECM components loss and compromised cartilage function [15, 16].The collagen network, predominantly composed of type II collagen fibrils, provides tensile strength and maintains the structural framework of cartilage [17]. Type IX and XI collagens cross-link with type II collagen to stabilize the fibrillar network [18]. Aging reduces type II collagen synthesis and increases type I collagen expression, which is less suited to cartilage function [19]. Collagen degradation is driven by matrix metalloproteinases (MMPs), particularly MMP-1 (collagenase-1), MMP-3 (stromelysin-1), and MMP-13 (collagenase-3) [20]. MMP-13, wich specifically degrades type II collagen, is highly upregulated in aging cartilage [21]. MMP expression is regulated by inflammatory cytokines (e.g., IL-1β, TNF-α) and oxidative stress, which activate transcription factors like NF-κB and AP-1 [22]. Advanced glycation end-products (AGEs) accumulate in collagen fibers through non-enzymatic reactions, forming cross-links that increase stiffness and reduce solubility [23]. AGEs interfere with normal collagen turnover, reducing susceptibility to collagenases and impairing ECM remodeling by chondrocytes [24]. These modifications weaken cartilage, making it less able to distribute loads and more vulnerable to microdamage [25]. Chondrocytes, the sole cellular component of cartilage, maintain ECM homeostasis by balancing synthesis and degradation [26, 27]. Aging chondrocytes undergo senescence, characterized by irreversible growth arrest, resistance to apoptosis, and the development of a senescence-associated secretory phenotype (SASP) [28]. Senescent chondrocytes exhibit high levels of cell cycle inhibitors (e.g. p16^INK4a and p21^CIP1) and accumulate DNA damage markers like γ-H2AX [29]. The SASP involves the secretion of pro-inflammatory cytokines (e.g., IL-6, IL-8), chemokines, growth factors, and proteases that create a pro-inflammatory microenvironment and promote ECM degradation [30]. Senescent chondrocytes increase production of MMPs and a disintegrin and metalloproteinase with thrombospondin motifs (ADAMTS), particularly ADAMTS-4 and ADAMTS-5, which degrade aggrecan [31]. At the same time, anabolic genes expression, including COL2A1 (type II collagen) and ACAN (aggrecan), declines due to transcriptional and epigenetic changes. This shift toward catabolism accelerate ECM breakdown [32, 33]. Oxidative stress results from an imbalance between the production of reactive oxygen species (ROS) and antioxidant defense capacity [34]. Chondrocytes generate ROS, such as superoxide anion (O₂•⁻), hydrogen peroxide (H₂O₂), and hydroxyl radicals (•OH), through mitochondrial electron transport chain leakage, NADPH oxidase activity, and inflammation. Aging impairs mitochondrial function, leading to increased ROS production and reduced ATP synthesis [35, 36]. ROS damage proteins, lipids, and DNA, impairing cellular functions and activating stress responses [34]. ROS-induced DNA damage triggers pathways involving p53 and other tumor suppressors, promoting cellular senescence. Additionally, ROS activate transcription factors like NF-κB and AP-1, which enhance the expression of pro-inflammatory cytokines (IL-1β, TNF-α), chemokines, and MMPs, creating a feedback loop that exacerbates oxidative stress and inflammation [37–39]. Chondrocytes have antioxidant systems, including superoxide dismutases (SOD1, SOD2), catalase, glutathione peroxidase, and thioredoxin reductase, which neutralize ROS. However, these defenses weaken with age, increasing susceptibility to oxidative damage and accelerating cartilage degeneration [40, 41].
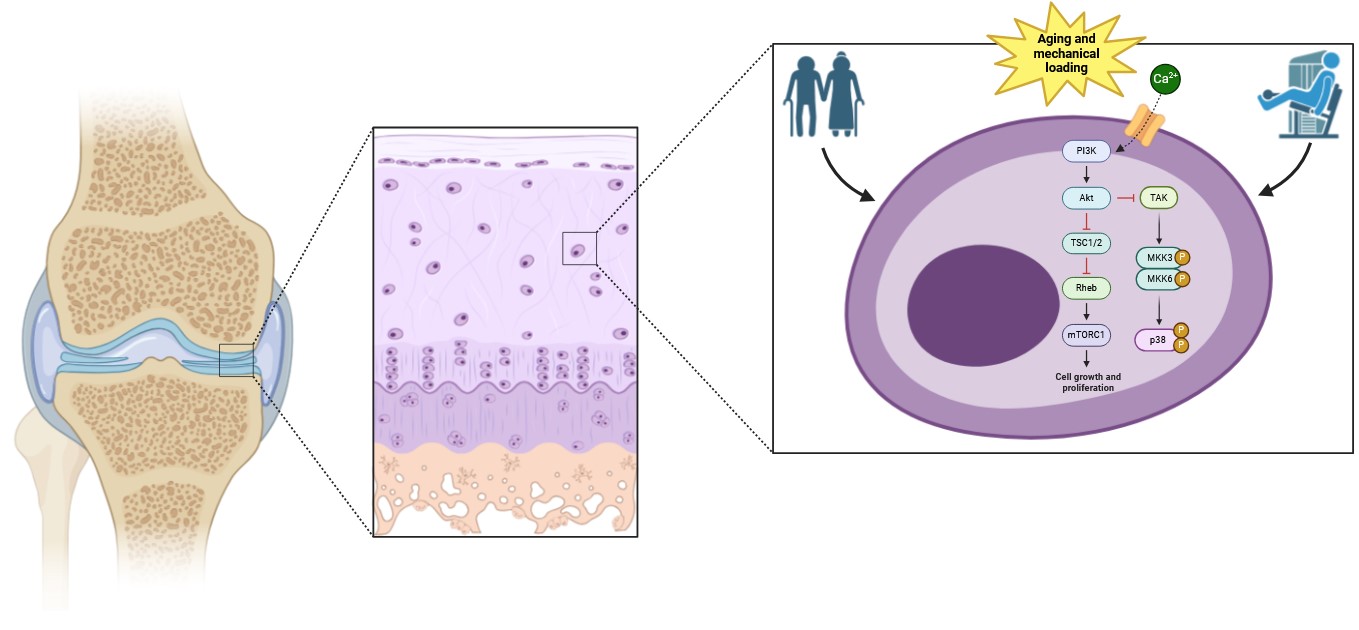
Fig. 1: Molecular Changes in Cartilage Aging and Mechanical Loading.
Aging cartilage exhibits chronic inflammation, often termed “inflammaging”, characterized by increased cytokines, chemokines, and degradative enzymes. Key mediators like IL-1β and TNF-α disrupt ECM homeostasis by stimulating MMPs and aggrecanases while inhibating anabolic pathways such us transforming growth factor-beta (TGF-β) and insulin-like growth factor-1 (IGF-1)[42, 43]. These cytokines activate NF-κB, MAPKs and JAK/STAT pathways driving inflammation and ECM degradation. Additionally, they induce nitric oxide (NO) production via inducible nitric oxide synthase (iNOS) and prostaglandin E₂ (PGE₂) via cyclooxygenase-2 (COX-2), contributing to chondrocyte apoptosis and further cartilage breakdown [35, 38, 44]. Mechanical loading regulates cartilage health via mechanotransduction—converting mechanical forces into biochemical signals. Chondrocytes sense mechanical stimuli through integrins, ion channels and cytoskeletal components. Integrins link the ECM to the intracellular actin cytoskeleton, activating signaling pathways such as PI3K/Akt and ERK, which support chondrocyte survival and ECM synthesis [45–48]. Stretch-activated ion channels (SACs), including TRPV4 and Piezo channels (Piezo1 and Piezo2), mediate calcium influx in response to mechanical stress. Intracellular calcium regulates cytoskeletal reorganization, gene expression, and anabolic activities essential for cartilage maintenance. However, aging impairs mechanosensitive ion channels declines, leading to defective calcium signaling and reduced chondrocyte responsiveness. Excessive mechanical stress activates p38 MAPK and JNK, upregulating catabolic enzymes and inflammatory mediators. Calcium overload can also trigger chondrocyte apoptosis via mitochondrial pathways [49–53]. The subchondral bone-cartilage interface is crucial for joint function. Aging increases subchondral bone stiffness, sclerosis, and microcracks, altering cartilage’s mechanical environment and promoting degradation [54–56]. Biochemical signals from subchondral bone cells, such as sclerostin and DKK1, inhibit the Wnt/β-catenin signaling in chondrocytes, impairing cartilage repair mechanisms. Altered vascularization and nutrient supply due to subchondral bone changes further contribute to cartilage degeneration [57–59]. Epigenetic changes, including DNA methylation, histone modifications, and non-coding RNA, regulate gene expression in aging cartilage. Methylation of anabolic genes (COL2A1 and ACAN) suppresses their expression, while demethylation of catabolic genes (MMP-13 and ADAMTS-5) promotes ECM degradation. Age-related alterations in histone modifications and miRNA profiles further contribute to cartilage degeneration [24, 60–64].
Treatment of cartilage lesions has made tremendous progress in recent years. Many techniques for regenerating the articular surface have been developed and positive outcomes have been validated at mid- and long-term follow-up examinations. Palliative treatments (such as chondroplasty), a wide range of regenerative procedures with varying degrees of complexity, and several bone-based cartilage resurfacing techniques are now in use. Bone marrow stimulation (BMS) procedures such as abrasion arthroplasty (AA), microfracture (MF) [2, 65–68], and autologous matrix-induced chondrogenesis (AMIC) are examples of regenerative therapies [1]. Autologous chondrocyte implantation (ACI) [69–73] and bone marrow aspirate concentration (BMAC) [74–76] are all cell-based procedures. Biological cartilage reconstruction, through osteochondral autograft transplantation and osteochondral allograft transplantation (OCA) [69, 77] as well as metallic and biosynthetic cartilage reconstruction through focal knee resurfacing implants (FKRIs) [78, 79], are all considered bone-based techniques because they rely on osseointegration rather than chondrogenesis [80]. These treatments together cover the current range of surgical options for cartilage restoration. However, these therapies do not usually consider the patient’s age [2, 81–83], and not all patients can be treated with these therapies with good results [69, 84]. Age has become one of the most commonly recognized features that is critical for treatment effectiveness [70–72, 85]. An upper age restriction is frequently used as an inclusion criterion in available studies evaluating the effectiveness of cartilage repair [86]. Despite the fact that 52% to 60% of cartilage procedures are performed on patients aged 40 to 60 years [2, 87], but common age limit for cartilage reconstruction surgery presented in the literature is 40 years (the ideal patient)[65, 72, 88]. As a result, middle-aged patients are underrepresented in research. Some studies have found that older patients perform poorly [70–72, 85]. It is hypothesized that aging has an adverse effect on articular cartilage by reducing its unique ability to regenerate [88]. The structure and composition of proteoglycans in cartilage also vary with age, reducing chondroitin sulfate concentration and the length of hyaluronate filament [70, 89]. These age-related changes may support an adverse reaction to treating older patients, while the true impact of these biological changes on patient symptoms and treatment outcomes remains still unknown [70]. One significant challenge in evaluating treatment outcomes in older patients is the reliance on patient-reported questionnaires, which are the most commonly used tools for assessing functional improvement. These questionnaires have limitations because lower scores in older patients may reflect age-related differences in baseline function rather than treatment efficacy. This introduces a potential bias, as healthy older individuals typically score lower than younger counterparts, even in the absence of pathology. Additionally, an active lifestyle plays a crucial role in cartilage repair outcomes [70].
An alternative approach for middle-aged and older patients involves regenerative therapies. Literature suggests that, in contrast to bone marrow stimulation techniques, which often exhibit reduced effectiveness in older patients due to declining therapeutic potential with aging, regenerative techniques may offer better outcomes in this patient group [65, 70]. Cell cultivation on scaffolds can lead to the activation of anabolic factors, inducing chondrocyte differentiation and reducing the expression and production of molecules involved in cartilage degeneration. This supports the potential use of bioengineered tissues to facilitate tissue repair, particularly in the treatment of older patients [70], such as the Hyalofast membrane used in this study. Consequently, autologous matrix-induced chondrogenesis (AMIC) has become popular in recent years. This approach involves the implantation of a biodegradable scaffold with microfractures. Due to its cost-effectiveness and efficiency, this method is increasingly used, with emerging clinical results indicating significant improvement in function and quality of life over medium- and long-term follow-up periods [90–93].
Among commercially available biocompatible scaffolds for cartilage repair, Hyalofast, which is also utilized in this study, stands out due to its three-dimensional structure and its bioactivity, biocompatibility, and biodegradability. It forms a matrix that serves as structural support for mesenchymal stem cells released by stimulated bones. Hyalofast promotes the proliferation and differentiation of these cells into chondrocytes. Moreover, during the degradation of this membrane, a higher amount of hyaluronic acid is released, creating a microenvironment that further facilitates the regeneration of damaged cartilage [90, 91, 94]. Currently, limited studies evaluate the short- and medium-term outcomes of treating knee chondral lesions with microfractures in combination with hyaluronic acid scaffold implantation, considering the wide variety of biological scaffolds available. This study aims to assess short- and medium-term clinical outcomes in patients aged 45 to 60 years with grade IV knee chondral lesions who underwent microfractures with hyaluronic acid scaffold implantation. Additionally, patients initiated an intensive rehabilitation program on the first day after the surgery. The outcomes were evaluated using subjective assessments by patients through two questionnaires (KOOS and SF-36) before the surgery, and at 6 and 12 months of follow-ups, alongside functional evaluation and MRI observations conducted by a qualified team. We hypothesize that the use of hyaluronic acid scaffolds and microfractures will lead to satisfactory clinical outcomes and facilitate an early return to daily activities in middle-aged patients.
Materials and Methods
Patient selection
The ICRS classification was used to categorize the patients for the surgery. A group of 16 middle-aged patients (8 men and 8 women; age range: 45-60 years; mean age: 55±8 years) had cartilage repair surgery. All of the patients were active both physically and professionally. As a result of traumatic damage, all patients developed lesions in the medial femoral condyle (MFC) (100%) and the laterial femoral condyle (LFC) (100%). The longest period of observation was 48 months (range: 24-48 months). Table 1 summarizes the characteristics of the patients involved in the research.
The research’s inclusion criteria were active middle-aged patients with IV grade articular cartilage degeneration who needed surgery. Patients under the age of 40 or above the age of 60 were excluded, as were those with muscular problems such as myasthenia gravis, progressive malnutrition, and periodic paralysis. Patients who refused to comply with therapy or refused to rehabilitate in the clinic under supervision were also excluded. Patients with abnormal bleeding or coagulation function, incomplete follow-up, imaging data, or a follow-up duration of less than 6 months were also barred from participation.
In this study, patients had a surgical intervention to deal with cartilage regeneration, which included the use of a Hyalofast membrane (Anika Therapeutics Inc., Bedford, MA, USA), microfractures, and tissue glue stabilisation. A comprehensive physical exam and MRI were conducted prior to surgery. During the examination, the patients had significant effusion, pain, and limited range of motion in the afflicted knee joint. The Lachmann and pivot shift tests gave positive results. The attending physician referred the patients for surgery after MRI (SIGNA 1.5T HDx; GE HealthCare Technologies Inc., Chicago, IL, USA) evaluation of the size and location of the lesion, assessment of pain intensity, and verification of the failure of conservative therapy. All patients who took part in the trial provided written informed consent.
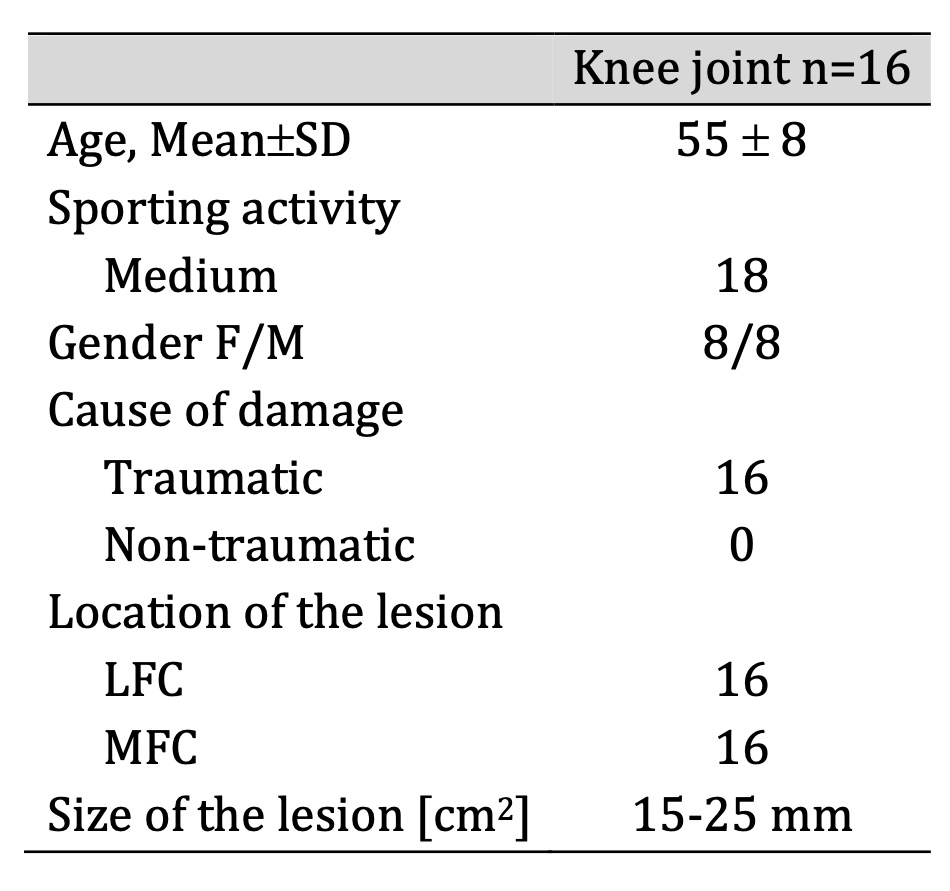
Table 1: Characteristics of the patients included in the study
Operation procedure
All surgical operations were conducted under general anesthesia by the same surgical team and physician. The procedure began with the placement of two anteromedial and anterolateral portals, followed by an extensive examination of the joint structures. After carefully removing the injured tissue, the size of the cartilage defect was assessed, and microfracture was done using specialized equipment at the base of the defect. The location had been cleansed for optimal visibility prior to the implantation of the Hyalofast membrane. The defect was filled with the patient’s blood before inserting a cannula and spreading a Hyalofast membrane across the surface using a needle and probe. After stabilizing the scaffold, the defect was filled with the individual’s blood sample and the Hyalofast membrane was fixed in place using TISSEEL Lyo tissue glue (Baxter International Inc., Deerfield, IL, USA). Patients were given anticoagulant medication after surgery (Neoparin 0.4/0.6 once daily for 20 days; SCIENCEPHARMA SP. Z O.O. SP.K., Warsaw, Poland). Furthermore, antibiotics (Clindamycin 600, every 8 hours; MIP PHARMA POLSKA SP. Z O.O., Gdask, Poland) were given for two weeks. It’s worth highlighting that no joint punctures or drains were used over the course of the therapy.
Follow-up evaluation
The research investigation intended to examine the treatment outcomes of individuals who had undergone surgery by comparing their preoperative status to a functional evaluation performed during follow-up visits. Before and after surgery, patients were requested to complete the SF-36 and Knee Osteoarthritis Outcome Score (KOOS) questionnaires. KOOS is an integrated test composed of five subscales that assess the intensity of pain (PAIN), symptoms (SYMPTOMS), daily living function (ADL), sports and recreational activity function (SPORT/REC), and quality of life (QOL) [95]. The SF-36 was developed to assess patients’ overall health and well-being, and it consists of eight areas that examine physical and mental performance function [96]. Furthermore, cartilage regeneration was examined using 1.5 T MRI images after an average of 6-8 weeks, 6 months, and 1 year. MRI offers a multidimensional examination of the joint with excellent sensitivity to soft tissue, allowing for an accurate assessment of the cartilage and its rebuilding process during subsequent follow-up visits [97, 98].
Rehabilitation protocol
During the post-operative rehabilitation time, no orthoses or external supports were needed. To treat edema and discomfort, a highly effective cooling system and compression stockings (GAME READY knee wrap (CoolSystems, Inc., Alpharetta, GA, USA), along with a regenerating and massaging system (Normatec (Hyper Ice, Inc., Irvine, CA, USA)) were applied. Rehab started with full weight bearing on the first surgical day, supported by elbow crutches. The crutches were taken away seven days later, and the patient’s full range of motion was maintained. The program for rehabilitation includes training with resistance, eccentric-concentric exercises, and full-body weight exercises, with an emphasis on improving both the erector and flexor muscles of the knee and increasing flexibility and range of motion. In unstable conditions, proprioception tasks were also incorporated. The workout routine, which included manual exercises, was supervised by a physiotherapist. Within three weeks resulting from surgery, the patients began preliminary training sessions under the supervision of a physiotherapist and a physician.
Statistics
The KOOS and SF-36 questionnaire findings were presented as mean values with standard deviation (SD). To evaluate statistical significance, a one-way analysis of variance (ANOVA) with repeated measures was performed to compare the differences between three time points: before treatment, 6 months after, and 12 months after. If the probability value (p) was less than 0.05, the results were considered statistically significant. To determine which time points significantly differed from each other, a Tukey’s post-hoc test was conducted. This test was chosen due to its robustness in handling multiple comparisons while controlling the family-wise error rate. To assess the clinical significance of the observed differences, Cohen’s d effect size was calculated for each comparison. The interpretation of Cohen’s d was based on standard thresholds (Small effect: 0.20 ≤ d ≤ 0.50; Medium effect: 0.50 ≤ d ≤ 0.80; Large effect: d ≥ 0.80)
Results
KOOS and SF-36 scale
The outcomes of patient assessments, as measured by two different questionnaires - KOOS and SF-36 are presented below. Tables 2 and 3 show the overall outcomes for every patient. The assessment of patients’ health status and quality of life using the KOOS and SF-36 questionnaires at six-month and one-year postoperative follow-up demonstrated a substantial improvement. The results showed favorable increases in a variety of parameters, including pain, symptoms, everyday activities, and sports-related metrics, indicating an overall improvement in patients’ well-being. The KOOS questionnaire results showed a significant improvement in all examined parameters. There was a substantial difference between the pre-surgery scores and those reported at the six-month and one-year follow-up examinations, showing that the surgical intervention was beneficial in improving patients’ health. Notably, the overall quality of life, as assessed by the KOOS scale, increased significantly, confirming the positive influence of the operation on patients’ well-being. Similarly, significant differences in several subscales were seen in the SF-36 questionnaire findings between the preoperative evaluation and the six-month and one-year postoperative evaluations. Changes were detected across all parameters measured by the SF-36 questionnaire at both time periods. The most significant increase was shown in the physical function area, showing a significant improvement in the patients’ ability to engage in physical activities. However, many characteristics, such as physical role, general health, emotional role, and mental health, had slightly lower ratings at the one-year follow-up compared to the six-month follow-up. These findings point to the necessity for ongoing monitoring and possibly intervention in certain areas (particularly physiotherapy and exercise) in order to maintain and enhance patients’ overall health and well-being.
The Cohen’s d results for KOOS questionnaires indicate that there was a large effect size observed across all measured domains—pain, symptoms, activities of daily living (ADL), sports/recreation, and quality of life (QOL)—both at 6 months and 12 months post-treatment. This suggests that the intervention led to significant and sustained improvements in all assessed aspects over time.
The Cohen’s d results for SF-36 questionnaires indicate the effect sizes of treatment outcomes at 6 months and 12 months across various health domains:
- Sustained large improvements were observed in Physical Function, Body Pain, and Mental Health, indicating significant benefits that persisted over time.
- Role-Physical, Vitality, and Role Emotional showed medium effects at both time points, suggesting moderate but stable improvements.
- General Health showed a medium effect at 6 months, but this reduced to small at 12 months, implying a decline in perceived general health benefits over time.
- Social Functioning improved from medium at 6 months to large at 12 months, indicating progressive benefits in social aspects of life.
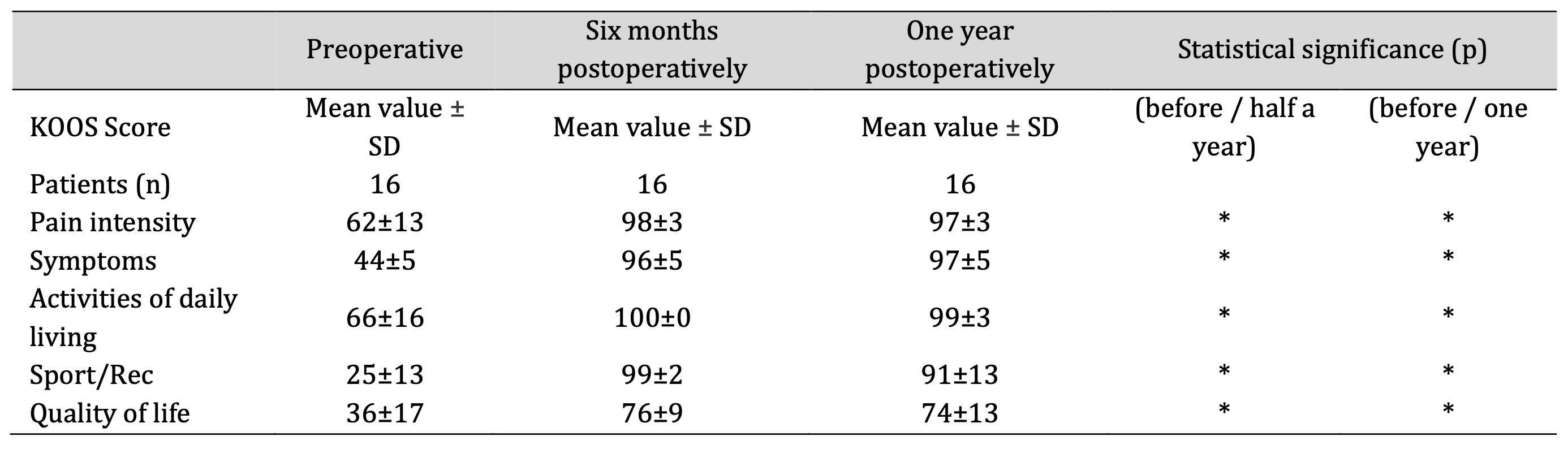
Table 2: Comparison of preoperative and postoperative result from KOOS questionnaires for all patients. Abbreviations: SD – standard deviation, *=statistical significance (p<0.05)
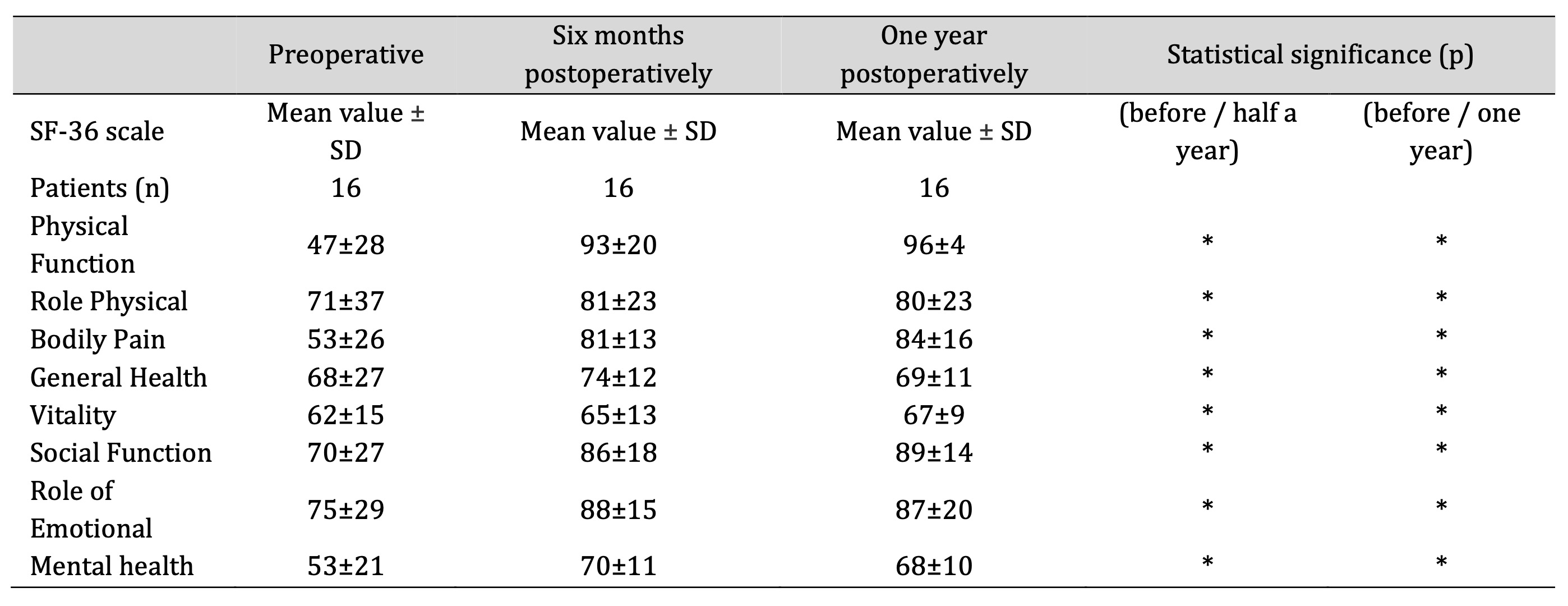
Table 3: Comparison of preoperative and postoperative results from the SF-36 questionnaires for all patients. Abbreviations: SD – standard deviation, *=statistical significance (p<0.05)
Functional assessment
The patient’s post-surgery recovery progress was outstanding, as they were able to resume normal daily activities within three to four weeks (Fig. 2). This suggests a satisfactory return of functional skills and a rapid postoperative rehabilitation procedure. Thorough assessments were performed during the six and twelve-month follow-up visits to evaluate the patient’s development. There were no abnormalities in terms of range of motion, edema, or discomfort in the operated joint, which was encouraging. These data indicate that the therapy intervention had a long-term favorable influence on the joint, allowing the patient to restore full mobility and function without any problems or side consequences. Joint mobility has been restored, which is necessary for carrying out everyday tasks and sustaining an active lifestyle. Furthermore, the lack of edema, or swelling, indicates that the healing process was effective and that the joint structures healed satisfactorily. Finally, the absence of pain during the follow-up visits illustrates the treatment’s success in relieving discomfort and increasing the patient’s overall quality of life.

Fig. 2: Patient during rehabilitation programme.
Radiological evaluation
To assess the effects of the therapy, all patients in the research had preoperative and postoperative magnetic resonance imaging (MRI). The outcomes obtained from all participants in the study were consistent. Fig. 3 shows a good example of these findings. A considerable decrease in the inflammatory response in the periosteum was found when preoperative and postoperative MRI images of cartilage were compared. The inflammatory reaction becomes unnoticeable, showing that the treatment has successfully managed the inflammatory process. This decrease in inflammation is a sign of treatment success and indicates that the conditions are suitable for cartilage regeneration. Furthermore, postoperative edema was reduced as measured by the subchondral layer. This decrease in subchondral layer edema is an essential indicator of the healing process. The decrease in edema indicates that wound healing and tissue regeneration are progressing, which is critical for the effective repair of cartilage abnormalities.
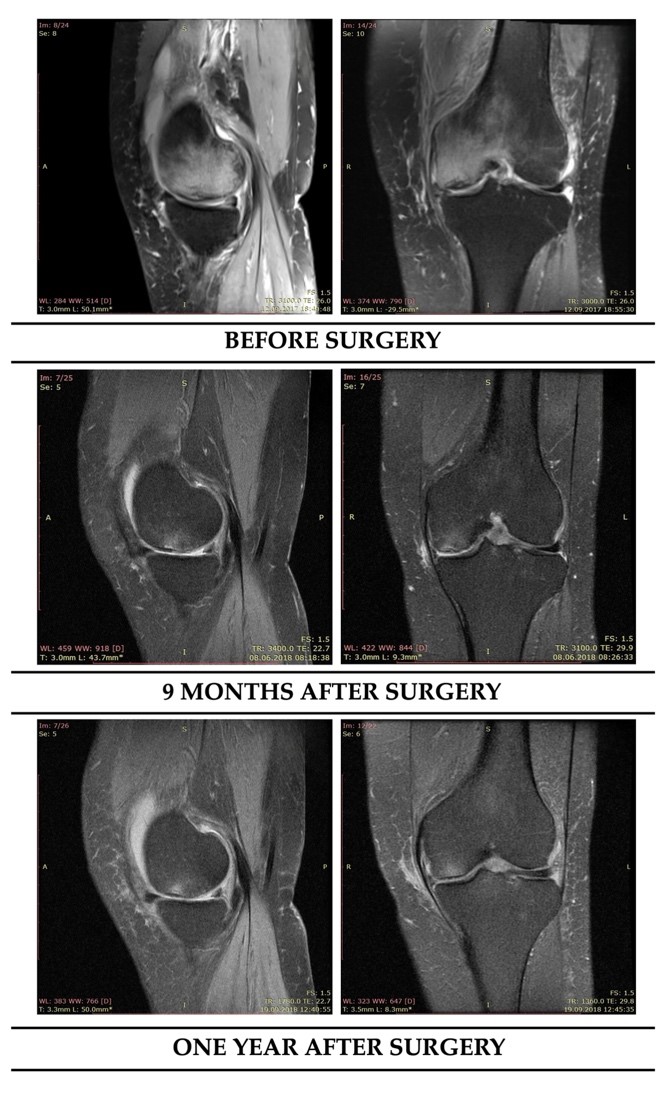
Fig. 3: Preoperative and one-year postoperative MRI examinations show progress of cartilage regeneration.
Discussion
Treating cartilage injuries in the population aged >45 remains a substantial clinical issue [99]. When a joint cartilage injury occurs, the resulting reparative fibrocartilage has poorer biological and biomechanical properties compared to native hyaline cartilage, and it may undergo degenerative changes, ultimately leading to osteoarthritis. For this reason, effective cartilage strategies are crucial [99, 100].
In this study, cartilage defects were treated in middle-aged individuals (age range: 45-60 years; mean age: 55±8 years) using the microfracture technique in combination with Hyalofast membrane. Our findings indicate that patient above 45 years experienced significant functional improvement, challenging the notion that age is a contraindication for this treatment. This contradicts previous studies, which typically report high failure rates of microfractures in older patients [99, 101–103], likely due to the age-related decline in regenerative potential of chondrocytes [104].
Age-dependent outcomes following microfractures for knee cartilage lesions have been widely studied. For instance, Steadman et al. [105] observed better outcomes in patients under 35, while Kreutz et al. [65] reported greater deterioration over time in those above 40. Similarly, Mithoefer et al. [106] and Knutsen et al. [107] found superior results on younger patients undergoing microfractures or autologous chondrocyte transplantations. These findings align with research suggesting that mesenchymal stem cells activity diminishes with age, potentially impairing cartilage repair [70, 108].
Despite these trends, some studies demonstrates that microfractures can still be beneficial in older populations. Miller’s et al. [109] applied the technique to 81 middle-aged patients and observed significant improvement, though some required additional procedures. Gobbi et al. [110] also found that while younger athletes had better outcomes, older individuals still benefited from treatment, suggesting that injury size may be a more critical factor than age alone.
A key factor distinguishing our study from prior work is the use of a hyaluronic acid-based scaffold (Hyalofast), which may have contributed to the superior clinical outcomes. Previous research has shown that scaffolds enhance cartilage regeneration by providing structural support and facilitating mesenchymal stem cell differentiation [111, 112]. Studies directly comparing microfractures with and without scaffolds demonstrate that scaffold-assisted treatments result in better defect filling and radiological improvement, supporting our observations [111–114]. Additionally, Tan et al. [93] reported significant health improvements in middle-aged patients treated with Hyalofast, reinforcing our findings.
However, our study has certain limitations. Firstly, the sample size was relatively small, which may impact the representativeness of the results. Additionally, our observations were limited to a short-term follow-up, so further studies are needed to evaluate the long-term effects of this therapy. Moreover, the study did not include a control group treated with microfractures alone, considering the well-being of the patients and the lower effectiveness of cartilage defect treatment with microfractures alone in older individuals.
Conclusion
In this study, we evaluated the outcomes of cartilage defect treatment in individuals aged 45 to 60 using the microfracture technique combined with the Hyalofast membrane. The primary objective was to assess the efficacy of this approach in improving joint function and quality of life in this age group. Our findings indicate that cartilage repair in middle-aged patients is not only feasible but also leads to significant clinical improvements. One of the key observations was the notable reduction in inflammatory symptoms surrounding the cartilage defect. Postoperative magnetic resonance imaging revealed that the inflammatory response was minimal or nearly absent, highlighting the treatment’s effectiveness in modulating inflammation—a crucial factor for tissue healing. Furthermore, we observed that the Hyalofast membrane successfully integrated with the surrounding cartilage structures, suggesting its potential to enhance cartilage repair and restore joint functionality. Another significant finding was the reduction of edema in the subchondral layer, indicating progressive wound healing. This aligns with expectations, as decreased edema is typically associated with improved tissue repair and cartilage regeneration. Overall, our results support the use of microfractures combined with a hyaluronic acid-based scaffold as an effective strategy for cartilage repair in middle-aged patients, potentially improving long-term joint health and functional outcomes.
Acknowledgements
Funding
This research received no external funding.
Institutional Review Board Statement
The study was carried out in accordance with the Declaration of Helsinki. The study did not require approval from the ethics committee. Only products with medical approval registrations were used in the study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. Data are not publicly available due to patient data protection.
Declaration of generative AI and AI-assisted technologies in the writing process
During the preparation of this work the authors used ChatGPT in order to improve readability and language. After using this tool/service, the authors reviewed and edited the content as needed and takes full responsibility for the content of the publication.
Disclosure Statement
The authors declare no Conflicts of Interest.
References
| 1 | Makris, E.A.; Gomoll, A.H.; Malizos, K.N.; Hu, J.C.; Athanasiou, K.A. Repair and Tissue Engineering Techniques for Articular Cartilage. Nat Rev Rheumatol 2015, 11, 21-34, doi:10.1038/NRRHEUM.2014.157.
https://doi.org/10.1038/nrrheum.2014.157 |
| 2 | Jeuken, R.M.; van Hugten, P.P.W.; Roth, A.K.; Timur, U.T.; Boymans, T.A.E.J.; van Rhijn, L.W.; Bugbee, W.D.; Emans, P.J. A Systematic Review of Focal Cartilage Defect Treatments In-Aged Versus Younger Patients. Orthop J Sports Med 2021, 9, doi:10.1177/23259671211031244.
https://doi.org/10.1177/23259671211031244 |
| 3 | Heir, S.; Nerhus, T.K.; Røtterud, J.H.; Løken, S.; Ekeland, A.; Engebretsen, L.; Årøen, A. Focal Cartilage Defects in the Knee Impair Quality of Life as Much as Severe Osteoarthritis: A Comparison of Knee Injury and Osteoarthritis Out-come Score in 4 Patient Categories Scheduled for Knee Surgery. Am J Sports Med 2010, 38, 231-237, doi:10.1177/0363546509352157.
https://doi.org/10.1177/0363546509352157 |
| 4 | Everhart, J.S.; Abouljoud, M.M.; Kirven, J.C.; Flanigan, D.C. Full-Thickness Cartilage Defects Are Important Independ-ent Predictive Factors for Progression to Total Knee Arthroplasty in Older Adults with Minimal to Moderate Osteo-arthritis: Data from the Osteoarthritis Initiative. J Bone Joint Surg Am 2019, 101, 56-63, doi:10.2106/JBJS.17.01657.
https://doi.org/10.2106/JBJS.17.01657 |
| 5 | Loeser, R. F. (2013). Aging processes and the development of osteoarthritis 1AD, 25(1), 108-113.
https://doi.org/10.1097/BOR.0b013e32835a9428 |
| 6 | Goldring, M. B., & Marcu, K. B. (2012). Epigenomic and microRNA-mediated regulation in cartilage development, homeostasis, and osteoarthritis 2AD, 18(2), 109-118.
https://doi.org/10.1016/j.molmed.2011.11.005 |
| 7 | Jeon, O.H.; Kim, C.; Laberge, R.M.; Demaria, M.; Rathod, S.; Vasserot, A.P.; Chung, J.W.; Kim, D.H.; Poon, Y.; David, N.; et al. Local Clearance of Senescent Cells Attenuates the Development of Post-Traumatic Osteoarthritis and Creates a pro-Regenerative Environment. Nature Medicine 2017 23:6 2017, 23, 775-781, doi:10.1038/nm.4324.
https://doi.org/10.1038/nm.4324 |
| 8 | Mobasheri, A.; Kalamegam, G.; Musumeci, G.; Batt, M.E. Chondrocyte and Mesenchymal Stem Cell-Based Therapies for Cartilage Repair in Osteoarthritis and Related Orthopaedic Conditions. Maturitas 2014, 78, 188-198, doi:10.1016/J.MATURITAS.2014.04.017.
https://doi.org/10.1016/j.maturitas.2014.04.017 |
| 9 | Bolduc, J.A.; Collins, J.A.; Loeser, R.F. Reactive Oxygen Species, Aging and Articular Cartilage Homeostasis. Free Radic Biol Med 2019, 132, 73-82, doi:10.1016/J.FREERADBIOMED.2018.08.038.
https://doi.org/10.1016/j.freeradbiomed.2018.08.038 |
| 10 | O'Conor, C.J.; Ramalingam, S.; Zelenski, N.A.; Benefield, H.C.; Rigo, I.; Little, D.; Wu, C.L.; Chen, D.; Liedtke, W.; McNulty, A.L.; et al. Cartilage-Specific Knockout of the Mechanosensory Ion Channel TRPV4 Decreases Age-Related Osteoarthritis. Sci Rep 2016, 6, doi:10.1038/SREP29053.
https://doi.org/10.1038/srep29053 |
| 11 | Henrotin, Y.E.; Bruckner, P.; Pujol, J.P.L. The Role of Reactive Oxygen Species in Homeostasis and Degradation of Cartilage. Osteoarthritis Cartilage 2003, 11, 747-755, doi:10.1016/S1063-4584(03)00150-X.
https://doi.org/10.1016/S1063-4584(03)00150-X |
| 12 | Rim, Y.A.; Nam, Y.; Ju, J.H. The Role of Chondrocyte Hypertrophy and Senescence in Osteoarthritis Initiation and Progression. International Journal of Molecular Sciences 2020, Vol. 21, Page 2358 2020, 21, 2358, doi:10.3390/IJMS21072358.
https://doi.org/10.3390/ijms21072358 |
| 13 | Vincent, T.L. Targeting Mechanotransduction Pathways in Osteoarthritis: A Focus on the Pericellular Matrix. Curr Opin Pharmacol 2013, 13, 449-454, doi:10.1016/J.COPH.2013.01.010.
https://doi.org/10.1016/j.coph.2013.01.010 |
| 14 | Stevens, E.B.; Stephens, G.J. Recent Advances in Targeting Ion Channels to Treat Chronic Pain. Br J Pharmacol 2018, 175, 2133, doi:10.1111/BPH.14215.
https://doi.org/10.1111/bph.14215 |
| 15 | Van Der Kraan, P.M. The Changing Role of TGFβ in Healthy, Ageing and Osteoarthritic Joints. Nat Rev Rheumatol 2017, 13, 155-163, doi:10.1038/NRRHEUM.2016.219.
https://doi.org/10.1038/nrrheum.2016.219 |
| 16 | Feng, R.; Hu, W.; Li, Y.; Yao, X.; Li, J.; Li, X.; Zhang, J.; Wu, Y.; Kang, F.; Dong, S. Mechanotransduction in Subchondral Bone Microenvironment and Targeted Interventions for Osteoarthritis. Mechanobiology in Medicine 2024, 2, 100043, doi:10.1016/J.MBM.2024.100043.
https://doi.org/10.1016/j.mbm.2024.100043 |
| 17 | Spyropoulou, A.; Karamesinis, K.; Basdra, E.K. Mechanotransduction Pathways in Bone Pathobiology. Biochim Bio-phys Acta 2015, 1852, 1700-1708, doi:10.1016/J.BBADIS.2015.05.010.
https://doi.org/10.1016/j.bbadis.2015.05.010 |
| 18 | Gardashli, M.; Baron, M.; Huang, C.; Kaplan, L.D.; Meng, Z.; Kouroupis, D.; Best, T.M. Mechanical Loading and Ortho-biologic Therapies in the Treatment of Post-Traumatic Osteoarthritis (PTOA): A Comprehensive Review. Front Bio-eng Biotechnol 2024, 12, 1401207, doi:10.3389/FBIOE.2024.1401207/BIBTEX.
https://doi.org/10.3389/fbioe.2024.1401207 |
| 19 | Zhu, S.; Zhu, J.; Zhen, G.; Hu, Y.; An, S.; Li, Y.; Zheng, Q.; Chen, Z.; Yang, Y.; Wan, M.; et al. Subchondral Bone Osteoclasts Induce Sensory Innervation and Osteoarthritis Pain. J Clin Invest 2019, 129, 1076-1093, doi:10.1172/JCI121561.
https://doi.org/10.1172/JCI121561 |
| 20 | Jacob, J.; Aggarwal, A.; Aggarwal, A.; Bhattacharyya, S.; Kumar, V.; Sharma, V.; Sahni, D. Senescent Chondrogenic Pro-genitor Cells Derived from Articular Cartilage of Knee Osteoarthritis Patients Contributes to Senescence-Associated Secretory Phenotype via Release of IL-6 and IL-8 Acta Histochem 2022, 124, doi:10.1016/J.ACTHIS.2022.151867.
https://doi.org/10.1016/j.acthis.2022.151867 |
| 21 | Chen, D.; Shen, J.; Zhao, W.; Wang, T.; Han, L.; Hamilton, J.L.; Im, H.J. Osteoarthritis: Toward a Comprehensive Under-standing of Pathological Mechanism. Bone Res 2017, 5, doi:10.1038/BONERES.2016.44.
https://doi.org/10.1038/boneres.2016.44 |
| 22 | Farr, J.N.; Khosla, S. Cellular Senescence in Bone. Bone 2019, 121, 121-133, doi:10.1016/J.BONE.2019.01.015.
https://doi.org/10.1016/j.bone.2019.01.015 |
| 23 | Kan, T.; Yu, Z.; Yan, M. Epigenetic Regulation of Chondrocytes Affected by Mitochondria through Mechanotransduc-tion in Osteoarthritis. Med Nov Technol Devices 2023, 18, 100230, doi:10.1016/J.MEDNTD.2023.100230.
https://doi.org/10.1016/j.medntd.2023.100230 |
| 24 | José Alcaraz, M. Control of Articular Degeneration by Extracellular Vesicles from Stem/Stromal Cells as a Potential Strategy for the Treatment of Osteoarthritis. Biochem Pharmacol 2024, 228, 116226, doi:10.1016/J.BCP.2024.116226.
https://doi.org/10.1016/j.bcp.2024.116226 |
| 25 | Price, J.S.; Waters, J.G.; Darrah, C.; Pennington, C.; Edwards, D.R.; Donell, S.T.; Clark, I.M. The Role of Chondrocyte Senescence in Osteoarthritis. Aging Cell 2002, 1, 57-65, doi:10.1046/J.1474-9728.2002.00008.X.
https://doi.org/10.1046/j.1474-9728.2002.00008.x |
| 26 | Barrett-Jolley, R.; Lewis, R.; Fallman, R.; Mobasheri, A. The Emerging Chondrocyte Channelome. Front Physiol 2010, 1 OCT, 2193, doi:10.3389/FPHYS.2010.00135/BIBTEX.
https://doi.org/10.3389/fphys.2010.00135 |
| 27 | Loeser, R.F.; Collins, J.A.; Diekman, B.O. Ageing and the Pathogenesis of Osteoarthritis. Nat Rev Rheumatol 2016, 12, 412-420, doi:10.1038/NRRHEUM.2016.65.
https://doi.org/10.1038/nrrheum.2016.65 |
| 28 | Li, G.; Yin, J.; Gao, J.; Cheng, T.S.; Pavlos, N.J.; Zhang, C.; Zheng, M.H. Subchondral Bone in Osteoarthritis: Insight into Risk Factors and Microstructural Changes. Arthritis Res Ther 2013, 15, doi:10.1186/AR4405.
https://doi.org/10.1186/ar4405 |
| 29 | Miyaki, S.; Asahara, H. Macro View of MicroRNA's Function in Osteoarthritis. Nat Rev Rheumatol 2012, 8, 543, doi:10.1038/NRRHEUM.2012.128.
https://doi.org/10.1038/nrrheum.2012.128 |
| 30 | Sekelova, T.; Danisovic, L.; Cehakova, M. Rejuvenation of Senescent Mesenchymal Stem Cells to Prevent Age-Related Changes in Synovial Joints. Cell Transplant 2023, 32, 09636897231200065, doi:10.1177/09636897231200065.
https://doi.org/10.1177/09636897231200065 |
| 31 | Durán-Sotuela, A.; Fernandez-Moreno, M.; Suárez-Ulloa, V.; Vázquez-García, J.; Relaño, S.; Hermida-Gómez, T.; Bal-boa-Barreiro, V.; Lourido-Salas, L.; Calamia, V.; Fernandez-Puente, P.; et al. A Meta-Analysis and a Functional Study Support the Influence of MtDNA Variant m.16519C on the Risk of Rapid Progression of Knee Osteoarthritis. Ann Rheum Dis 2023, 82, 974-984, doi:10.1136/ARD-2022-223570.
https://doi.org/10.1136/ard-2022-223570 |
| 32 | Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745-1759, doi:10.1016/S0140-6736(19)30417-9.
https://doi.org/10.1016/S0140-6736(19)30417-9 |
| 33 | Zeng, C.Y.; Wang, X.F.; Hua, F.Z. HIF-1α in Osteoarthritis: From Pathogenesis to Therapeutic Implications. Front Phar-macol 2022, 13, 927126, doi:10.3389/FPHAR.2022.927126.
https://doi.org/10.3389/fphar.2022.927126 |
| 34 | Qin, Y.-X.; Zhao, J. Mechanobiology in Cellular, Molecular, and Tissue Adaptation. Mechanobiology in Medicine 2023, 1, 100022, doi:10.1016/J.MBM.2023.100022.
https://doi.org/10.1016/j.mbm.2023.100022 |
| 35 | Jiang, Y. Osteoarthritis Year in Review 2021: Biology. Osteoarthritis Cartilage 2022, 30, 207-215, doi:10.1016/J.JOCA.2021.11.009.
https://doi.org/10.1016/j.joca.2021.11.009 |
| 36 | Mobasheri, A.; Matta, C.; Uzielienè, I.; Budd, E.; Martín-Vasallo, P.; Bernotiene, E. The Chondrocyte Channelome: A Narrative Review. Joint Bone Spine 2019, 86, 29-35, doi:10.1016/J.JBSPIN.2018.01.012.
https://doi.org/10.1016/j.jbspin.2018.01.012 |
| 37 | Segarra-Queralt, M.; Crump, K.; Pascuet-Fontanet, A.; Gantenbein, B.; Noailly, J. The Interplay between Biochemical Mediators and Mechanotransduction in Chondrocytes: Unravelling the Differential Responses in Primary Knee Os-teoarthritis. Phys Life Rev 2024, 48, 205-221, doi:10.1016/J.PLREV.2024.02.003.
https://doi.org/10.1016/j.plrev.2024.02.003 |
| 38 | Ren, X.; Zhuang, H.; Li, B.; Jiang, F.; Zhang, Y.; Zhou, P. Gsmtx4 Alleviated Osteoarthritis through Pie-zo1/Calcineurin/NFAT1 Signaling Axis under Excessive Mechanical Strain. Int J Mol Sci 2023, 24, doi:10.3390/IJMS24044022.
https://doi.org/10.3390/ijms24044022 |
| 39 | Gao, W.; Hasan, H.; Anderson, D.E.; Lee, W. The Role of Mechanically-Activated Ion Channels Piezo1, Piezo2, and TRPV4 in Chondrocyte Mechanotransduction and Mechano-Therapeutics for Osteoarthritis. Front Cell Dev Biol 2022, 10, 885224, doi:10.3389/FCELL.2022.885224/BIBTEX.
https://doi.org/10.3389/fcell.2022.885224 |
| 40 | Hodgkinson, T.; Amado, I.N.; O'Brien, F.J.; Kennedy, O.D. The Role of Mechanobiology in Bone and Cartilage Model Systems in Characterizing Initiation and Progression of Osteoarthritis. APL Bioeng 2022, 6, doi:10.1063/5.0068277.
https://doi.org/10.1063/5.0068277 |
| 41 | Savadipour, A.; Palmer, D.; Ely, E. V.; Collins, K.H.; Garcia-Castorena, J.M.; Harissa, Z.; Kim, Y.S.; Oestrich, A.; Qu, F.; Ra-shidi, N.; et al. The Role of PIEZO Ion Channels in the Musculoskeletal System. Am J Physiol Cell Physiol 2023, 324, C728-C740, doi:10.1152/AJPCELL.00544.2022.
https://doi.org/10.1152/ajpcell.00544.2022 |
| 42 | Jiang, W.; Chen, H.; Lin, Y.; Cheng, K.; Zhou, D.; Chen, R.; Song, C.; Zeng, L.; Yu, H. Mechanical Stress Abnormalities Promote Chondrocyte Senescence - The Pathogenesis of Knee Osteoarthritis. Biomed Pharmacother 2023, 167, doi:10.1016/J.BIOPHA.2023.115552.
https://doi.org/10.1016/j.biopha.2023.115552 |
| 43 | Wang, S.; Li, W.; Zhang, P.; Wang, Z.; Ma, X.; Liu, C.; Vasilev, K.; Zhang, L.; Zhou, X.; Liu, L.; et al. Mechanical Overloading Induces GPX4-Regulated Chondrocyte Ferroptosis in Osteoarthritis via Piezo1 Channel Facilitated Calcium Influx. J Adv Res 2022, 41, 63-75, doi:10.1016/J.JARE.2022.01.004.
https://doi.org/10.1016/j.jare.2022.01.004 |
| 44 | Wang, M.; Sampson, E.R.; Jin, H.; Li, J.; Ke, Q.H.; Im, H.J.; Chen, D. MMP13 Is a Critical Target Gene during the Progres-sion of Osteoarthritis. Arthritis Res Ther 2013, 15, doi:10.1186/AR4133.
https://doi.org/10.1186/ar4133 |
| 45 | Deng, Z.; Chen, X.; Lin, Z.; Alahdal, M.; Wang, D.; Liu, J.; Li, W. The Homeostasis of Cartilage Matrix Remodeling and the Regulation of Volume-Sensitive Ion Channel. Aging Dis 2022, 13, 787-800, doi:10.14336/AD.2021.1122.
https://doi.org/10.14336/AD.2021.1122 |
| 46 | Seol, D.; McCabe, D.J.; Choe, H.; Zheng, H.; Yu, Y.; Jang, K.; Walter, M.W.; Lehman, A.D.; Ding, L.; Buckwalter, J.A.; et al. Chondrogenic Progenitor Cells Respond to Cartilage Injury. Arthritis Rheum 2012, 64, 3626-3637, doi:10.1002/ART.34613.
https://doi.org/10.1002/art.34613 |
| 47 | Caramés, B.; Taniguchi, N.; Otsuki, S.; Blanco, F.J.; Lotz, M. Autophagy Is a Protective Mechanism in Normal Cartilage, and Its Aging-Related Loss Is Linked with Cell Death and Osteoarthritis. Arthritis Rheum 2010, 62, 791-801, doi:10.1002/ART.27305.
https://doi.org/10.1002/art.27305 |
| 48 | Yuan, X.L.; Meng, H.Y.; Wang, Y.C.; Peng, J.; Guo, Q.Y.; Wang, A.Y.; Lu, S.B. Bone-Cartilage Interface Crosstalk in Osteo-arthritis: Potential Pathways and Future Therapeutic Strategies. Osteoarthritis Cartilage 2014, 22, 1077-1089, doi:10.1016/J.JOCA.2014.05.023.
https://doi.org/10.1016/j.joca.2014.05.023 |
| 49 | He, Z.; Yan, Z.; Zhang, Y.; Xv, Y.; Chen, K.; Zhan, J.; Zhang, Y. Excessive Mechanical Stress Mediated Piezo1 Activation Regulates Lysosomal Membrane Permeabilization-Induced Chondrocyte Apoptosis in Mouse Osteoarthritis Model. 2022, doi:10.21203/RS.3.RS-2237583/V1.
https://doi.org/10.21203/rs.3.rs-2237583/v1 |
| 50 | Fang, T.; Zhou, X.; Jin, M.; Nie, J.; Li, Xi.I. Molecular Mechanisms of Mechanical Load-Induced Osteoarthritis. Int Or-thop 2021, 45, 1125-1136, doi:10.1007/S00264-021-04938-1.
https://doi.org/10.1007/s00264-021-04938-1 |
| 51 | Buckwalter, J.A.; Brown, T.D. Joint Injury, Repair, and Remodeling: Roles in Post-Traumatic Osteoarthritis | Request PDF. Clin Orthop Relat Res 2004, 423, 7-16.
https://doi.org/10.1097/01.blo.0000131638.81519.de |
| 52 | Zhou, R.; Fu, W.; Vasylyev, D.; Waxman, S.G.; Liu, C.J. Ion Channels in Osteoarthritis: Emerging Roles and Potential Targets. Nat Rev Rheumatol 2024, 20, 545-564, doi:10.1038/S41584-024-01146-0.
https://doi.org/10.1038/s41584-024-01146-0 |
| 53 | Charlier, E.; Deroyer, C.; Ciregia, F.; Malaise, O.; Neuville, S.; Plener, Z.; Malaise, M.; de Seny, D. Chondrocyte Dedif-ferentiation and Osteoarthritis (OA). Biochem Pharmacol 2019, 165, 49-65, doi:10.1016/J.BCP.2019.02.036.
https://doi.org/10.1016/j.bcp.2019.02.036 |
| 54 | Lotz, M.K.; Otsuki, S.; Grogan, S.P.; Sah, R.; Terkeltaub, R.; D'Lima, D. Cartilage Cell Clusters. Arthritis Rheum 2010, 62, 2206-2218, doi:10.1002/ART.27528.
https://doi.org/10.1002/art.27528 |
| 55 | Lotz, M.K.; Caramés, B. Autophagy and Cartilage Homeostasis Mechanisms in Joint Health, Aging and Osteoarthritis. Nat Rev Rheumatol 2011, 7, 579, doi:10.1038/NRRHEUM.2011.109.
https://doi.org/10.1038/nrrheum.2011.109 |
| 56 | Neefjes, M.; van Caam, A.P.M.; van der Kraan, P.M. Transcription Factors in Cartilage Homeostasis and Osteoarthritis. Biology (Basel) 2020, 9, 290, doi:10.3390/BIOLOGY9090290.
https://doi.org/10.3390/biology9090290 |
| 57 | Blanco, F.J.; Rego, I.; Ruiz-Romero, C. The Role of Mitochondria in Osteoarthritis. Nat Rev Rheumatol 2011, 7, 161-169, doi:10.1038/NRRHEUM.2010.213.
https://doi.org/10.1038/nrrheum.2010.213 |
| 58 | Figueroa, P.L.D. The Role of Autophagy in Aging-Related Osteoarthritis. 2017.
|
| 59 | Lawson, M.G.; Ritchison, H.M. Molecular Basis of Senescence in Osteoarthritis. Asia-Pacific Journal of Surgical & Experimental Pathology 2024, doi:10.32948/AJSEP.2024.11.22.
https://doi.org/10.32948/ajsep.2024.11.22 |
| 60 | Wang, H.; Yuan, T.; Wang, Y.; Liu, C.; Li, D.; Li, Z.; Sun, S. Osteoclasts and Osteoarthritis: Novel Intervention Targets and Therapeutic Potentials during Aging. Aging Cell 2024, 23, e14092, doi:10.1111/ACEL.14092.
https://doi.org/10.1111/acel.14092 |
| 61 | Rizzo, M.G.; Best, T.M.; Huard, J.; Philippon, M.; Hornicek, F.; Duan, Z.; Griswold, A.J.; Kaplan, L.D.; Hare, J.M.; Kou-roupis, D. Therapeutic Perspectives for Inflammation and Senescence in Osteoarthritis Using Mesenchymal Stem Cells, Mesenchymal Stem Cell-Derived Extracellular Vesicles and Senolytic Agents. Cells 2023, 12, doi:10.3390/CELLS12101421.
https://doi.org/10.3390/cells12101421 |
| 62 | Fu, B.; Shen, J.; Zou, X.; Sun, N.; Zhang, Z.; Liu, Z.; Zeng, C.; Liu, H.; Huang, W. Matrix Stiffening Promotes Chondrocyte Senescence and the Osteoarthritis Development through Downregulating HDAC3 Bone Res 2024, 12, doi:10.1038/S41413-024-00333-9.
https://doi.org/10.1038/s41413-024-00333-9 |
| 63 | Li, X.; Gibson, G.; Kim, J.S.; Kroin, J.; Xu, S.; van Wijnen, A.J.; Im, H.J. MicroRNA-146a Is Linked to Pain-Related Patho-physiology of Osteoarthritis. Gene 2011, 480, 34-41, doi:10.1016/J.GENE.2011.03.003.
https://doi.org/10.1016/j.gene.2011.03.003 |
| 64 | Wang, F.S.; Wu, R.W.; Chen, Y.S.; Ko, J.Y.; Jahr, H.; Lian, W.S. Biophysical Modulation of the Mitochondrial Metabolism and Redox in Bone Homeostasis and Osteoporosis: How Biophysics Converts into Bioenergetics. Antioxidants (Ba-sel) 2021, 10, doi:10.3390/ANTIOX10091394.
https://doi.org/10.3390/antiox10091394 |
| 65 | Kreuz, P.C.; Erggelet, C.; Steinwachs, M.R.; Krause, S.J.; Lahm, A.; Niemeyer, P.; Ghanem, N.; Uhl, M.; Südkamp, N. Is Microfracture of Chondral Defects in the Knee Associated with Different Results in Patients Aged 40 Years or Younger? Arthroscopy 2006, 22, 1180-1186, doi:10.1016/J.ARTHRO.2006.06.020.
https://doi.org/10.1016/j.arthro.2006.06.020 |
| 66 | McCormick, F.; Harris, J.D.; Abrams, G.D.; Frank, R.; Gupta, A.; Hussey, K.; Wilson, H.; Bach, B.; Cole, B. Trends in the Surgical Treatment of Articular Cartilage Lesions in the United States: An Analysis of a Large Private-Payer Database over a Period of 8 Years. Arthroscopy 2014, 30, 222-226, doi:10.1016/J.ARTHRO.2013.11.001.
https://doi.org/10.1016/j.arthro.2013.11.001 |
| 67 | Montgomery, S.R.; Foster, B.D.; Ngo, S.S.; Terrell, R.D.; Wang, J.C.; Petrigliano, F.A.; McAllister, D.R. Trends in the Surgi-cal Treatment of Articular Cartilage Defects of the Knee in the United States. Knee Surg Sports Traumatol Arthrosc 2014, 22, 2070-2075, doi:10.1007/S00167-013-2614-9.
https://doi.org/10.1007/s00167-013-2614-9 |
| 68 | Sansone, V.; De Girolamo, L.; Pascale, W.; Melato, M.; Pascale, V. Long-Term Results of Abrasion Arthroplasty for Full-Thickness Cartilage Lesions of the Medial Femoral Condyle. Arthroscopy 2015, 31, 396-403, doi:10.1016/J.ARTHRO.2014.10.007.
https://doi.org/10.1016/j.arthro.2014.10.007 |
| 69 | Brix, M.O.; Stelzeneder, D.; Chiari, C.; Koller, U.; Nehrer, S.; Dorotka, R.; Windhager, R.; Domayer, S.E. Treatment of Full-Thickness Chondral Defects With Hyalograft C in the Knee: Long-Term Results. Am J Sports Med 2014, 42, 1426-1432, doi:10.1177/0363546514526695.
https://doi.org/10.1177/0363546514526695 |
| 70 | Filardo, G.; Andriolo, L.; Sessa, A.; Vannini, F.; Ferruzzi, A.; Marcacci, M.; Kon, E. Age Is Not a Contraindication for Carti-lage Surgery: A Critical Analysis of Standardized Outcomes at Long-Term Follow-Up. Am J Sports Med 2017, 45, 1822-1828, doi:10.1177/0363546517695088.
https://doi.org/10.1177/0363546517695088 |
| 71 | Filardo, G.; Kon, E.; Andriolo, L.; Di Matteo, B.; Balboni, F.; Marcacci, M. Clinical Profiling in Cartilage Regeneration: Prognostic Factors for Midterm Results of Matrix-Assisted Autologous Chondrocyte Transplantation. Am J Sports Med 2014, 42, 898-905, doi:10.1177/0363546513518552.
https://doi.org/10.1177/0363546513518552 |
| 72 | Krishnan, S.P.; Skinner, J.A.; Bartlett, W.; Carrington, R.W.J.; Flanagan, A.M.; Briggs, T.W.R.; Bentley, G. Who Is the Ideal Candidate for Autologous Chondrocyte Implantation? J Bone Joint Surg Br 2006, 88, 61-64, doi:10.1302/0301-620X.88B1.16796.
https://doi.org/10.1302/0301-620X.88B1.16796 |
| 73 | Niemeyer, P.; Köstler, W.; Salzmann, G.M.; Lenz, P.; Kreuz, P.C.; Südkamp, N.P. Autologous Chondrocyte Implantation for Treatment of Focal Cartilage Defects in Patients Age 40 Years and Older: A Matched-Pair Analysis with 2-Year Fol-low-Up. Am J Sports Med 2010, 38, 2410-2416, doi:10.1177/0363546510376742.
https://doi.org/10.1177/0363546510376742 |
| 74 | Gobbi, A.; Karnatzikos, G.; Sankineani, S.R. One-Step Surgery with Multipotent Stem Cells for the Treatment of Large Full-Thickness Chondral Defects of the Knee. Am J Sports Med 2014, 42, 648-657, doi:10.1177/0363546513518007.
https://doi.org/10.1177/0363546513518007 |
| 75 | Gobbi, A.; Scotti, C.; Karnatzikos, G.; Mudhigere, A.; Castro, M.; Peretti, G.M. One-Step Surgery with Multipotent Stem Cells and Hyaluronan-Based Scaffold for the Treatment of Full-Thickness Chondral Defects of the Knee in Pa-tients Older than 45 Years. Knee Surg Sports Traumatol Arthrosc 2017, 25, 2494-2501, doi:10.1007/S00167-016-3984-6.
https://doi.org/10.1007/s00167-016-3984-6 |
| 76 | Nejadnik, H.; Hui, J.H.; Choong, E.P.F.; Tai, B.C.; Eng Hin Lee Autologous Bone Marrow-Derived Mesenchymal Stem Cells versus Autologous Chondrocyte Implantation: An Observational Cohort Study. Am J Sports Med 2010, 38, 1110-1116, doi:10.1177/0363546509359067.
https://doi.org/10.1177/0363546509359067 |
| 77 | Anderson, D.E.; Robinson, K.S.; Wiedrick, J.; Crawford, D.C. Efficacy of Fresh Osteochondral Allograft Transplantation in the Knee for Adults 40 Years and Older. Orthop J Sports Med 2018, 6, doi:10.1177/2325967118805441.
https://doi.org/10.1177/2325967118805441 |
| 78 | Holz, J.; Spalding, T.; Boutefnouchet, T.; Emans, P.; Eriksson, K.; Brittberg, M.; Konradsen, L.; Kösters, C.; Verdonk, P.; Högström, M.; et al. Patient-Specific Metal Implants for Focal Chondral and Osteochondral Lesions in the Knee; Ex-cellent Clinical Results at 2 Years. Knee Surg Sports Traumatol Arthrosc 2021, 29, 2899-2910, doi:10.1007/S00167-020-06289-7.
https://doi.org/10.1007/s00167-020-06289-7 |
| 79 | Martinez-Carranza, N.; Rockborn, P.; Roberts, D.; Högström, M.; Stålman, A. Successful Treatment of Femoral Chon-dral Lesions with a Novel Customized Metal Implant at Midterm Follow-Up. Cartilage 2021, 13, 1726S-1733S, doi:10.1177/1947603520967064.
https://doi.org/10.1177/1947603520967064 |
| 80 | McCarty, E.C.; Fader, R.R.; Mitchell, J.J.; Glenn, R.E.; Potter, H.G.; Spindler, K.P. Fresh Osteochondral Allograft Versus Autograft: Twelve-Month Results in Isolated Canine Knee Defects. Am J Sports Med 2016, 44, 2354-2365, doi:10.1177/0363546516648700.
https://doi.org/10.1177/0363546516648700 |
| 81 | Alford, J.W.; Cole, B.J. Cartilage Restoration, Part 2: Techniques, Outcomes, and Future Directions. Am J Sports Med 2005, 33, 443-460, doi:10.1177/0363546505274578.
https://doi.org/10.1177/0363546505274578 |
| 82 | Biant, L.C.; McNicholas, M.J.; Sprowson, A.P.; Spalding, T. The Surgical Management of Symptomatic Articular Cartilage Defects of the Knee: Consensus Statements from United Kingdom Knee Surgeons. Knee 2015, 22, 446-449, doi:10.1016/J.KNEE.2015.06.001.
https://doi.org/10.1016/j.knee.2015.06.001 |
| 83 | Henn, R.F.; Gomoll, A.H. A Review of the Evaluation and Management of Cartilage Defects in the Knee. Physician and Sportsmedicine 2011, 39, 101-107, doi:10.3810/psm.2011.02.1867.
https://doi.org/10.3810/psm.2011.02.1867 |
| 84 | Peterson, L.; Vasiliadis, H.S.; Brittberg, M.; Lindahl, A. Autologous Chondrocyte Implantation: A Long-Term Follow-Up. Am J Sports Med 2010, 38, 1117-1124, doi:10.1177/0363546509357915.
https://doi.org/10.1177/0363546509357915 |
| 85 | De Windt, T.S.; Bekkers, J.E.J.; Creemers, L.B.; Dhert, W.J.A.; Saris, D.B.F. Patient Profiling in Cartilage Regeneration: Prognostic Factors Determining Success of Treatment for Cartilage Defects. Am J Sports Med 2009, 37 Suppl 1, 58S-62S, doi:10.1177/0363546509349765.
https://doi.org/10.1177/0363546509349765 |
| 86 | Engen, C.N.; Engebretsen, L.; Årøen, A. Knee Cartilage Defect Patients Enrolled in Randomized Controlled Trials Are Not Representative of Patients in Orthopedic Practice. Cartilage 2010, 1, 312-319, doi:10.1177/1947603510373917.
https://doi.org/10.1177/1947603510373917 |
| 87 | Gowd, A.K.; Cvetanovich, G.L.; Liu, J.N.; Christian, D.R.; Cabarcas, B.C.; Redondo, M.L.; Verma, N.N.; Yanke, A.B.; Cole, B.J. Management of Chondral Lesions of the Knee: Analysis of Trends and Short-Term Complications Using the Na-tional Surgical Quality Improvement Program Database. Arthroscopy 2019, 35, 138-146, doi:10.1016/J.ARTHRO.2018.07.049.
https://doi.org/10.1016/j.arthro.2018.07.049 |
| 88 | Kon, E.; Filardo, G.; Condello, V.; Collarile, M.; Di Martino, A.; Zorzi, C.; Marcacci, M. Second-Generation Autologous Chondrocyte Implantation: Results in Patients Older than 40 Years. Am J Sports Med 2011, 39, 1668-1675, doi:10.1177/0363546511404675.
https://doi.org/10.1177/0363546511404675 |
| 89 | Plaas, A.H.K.; Sandy, J.D. Age-Related Decrease in the Link-Stability of Proteoglycan Aggregates Formed by Articular Chondrocytes. Biochem J 1984, 220, 337-340, doi:10.1042/BJ2200337.
https://doi.org/10.1042/bj2200337 |
| 90 | Jaramillo Quiceno, G.A.; Sarmiento Riveros, P.A.; Ochoa Perea, G.A.; Vergara, M.G.; Rodriguez Muñoz, L.F.; Arias Pe-rez, R.D.; Piovesan, N.O.; Muñoz Salamanca, J.A. Satisfactory Clinical Outcomes with Autologous Matrix-Induced Chondrogenesis in the Treatment of Grade IV Chondral Injuries of the Knee. Journal of ISAKOS 2023, 8, 86-93, doi:10.1016/J.JISAKO.2022.11.004.
https://doi.org/10.1016/j.jisako.2022.11.004 |
| 91 | Banerjee, S.; Sahanand, K.S. Managing Chondral Lesions: A Literature Review and Evidence-Based Clinical Guidelines. Indian J Orthop 2021, 55, 252-262, doi:10.1007/S43465-021-00355-Z.
https://doi.org/10.1007/s43465-021-00355-z |
| 92 | Chou, A.; Lie, D. A Technique Using a Low-Cost, Accessible Cannula to Aid Scaffold Passage in Dry Arthroscopic Carti-lage Repair in the Knee. Arthrosc Tech 2020, 9, e775, doi:10.1016/J.EATS.2020.02.009.
https://doi.org/10.1016/j.eats.2020.02.009 |
| 93 | Tan, S.I.; Tho, S.J.W.; Tho, K.S. Biological Resurfacing of Grade IV Articular Cartilage Ulcers in Knee Joint with Hyalofast. Journal of Orthopaedic Surgery 2020, 28, doi:10.1177/2309499020905158/ASSET/IMAGES/LARGE/10.1177_2309499020905158-FIG3.JPEG.
https://doi.org/10.1177/2309499020905158 |
| 94 | Karpinski, K.; Häner, M.; Bierke, S.; Petersen, W. Matrix-Induced Chondrogenesis Is a Valid and Safe Cartilage Repair Option for Small- to Medium-Sized Cartilage Defects of the Knee: A Systematic Review. Knee Surgery, Sports Trau-matology, Arthroscopy 2021, 29, 4213-4222, doi:10.1007/S00167-021-06513-Y/METRICS.
https://doi.org/10.1007/s00167-021-06513-y |
| 95 | Roos, E.M.; Roos, H.P.; Lohmander, L.S.; Ekdahl, C.; Beynnon, B.D. Knee Injury and Osteoarthritis Outcome Score (KOOS)-Development of a Self-Administered Outcome Measure. https://doi.org/10.2519/jospt.1998.28.2.88 1998, 28, 88-96, doi:10.2519/JOSPT.1998.28.2.88.
https://doi.org/10.2519/jospt.1998.28.2.88 |
| 96 | Ware, J.E. SF-36 Health Survey Update. Spine (Phila Pa 1976) 2000, 25, 3130-3139, doi:10.1097/00007632-200012150-00008.
https://doi.org/10.1097/00007632-200012150-00008 |
| 97 | Brown, W.E.; Potter, H.G.; Marx, R.G.; Wickiewicz, T.L.; Warren, R.F. Magnetic Resonance Imaging Appearance of Cartilage Repair in the Knee. Clin Orthop Relat Res 2004, 422, 214-223, doi:10.1097/01.BLO.0000129162.36302.4F.
https://doi.org/10.1097/01.blo.0000129162.36302.4f |
| 98 | Disler, D.G.; McCauley, T.R.; Kelman, C.G.; Fuchs, M.D.; Ratner, L.M.; Wirth, C.R.; Hospodar, P.P. Fat-Suppressed Three-Dimensional Spoiled Gradient-Echo MR Imaging of Hyaline Cartilage Defects in the Knee: Comparison with Standard MR Imaging and Arthroscopy. AJR Am J Roentgenol 1996, 167, 127-132, doi:10.2214/AJR.167.1.8659356.
https://doi.org/10.2214/ajr.167.1.8659356 |
| 99 | Gobbi, A.; Scotti, C.; Karnatzikos, G.; Mudhigere, A.; Castro, M.; Peretti, G.M. One-Step Surgery with Multipotent Stem Cells and Hyaluronan-Based Scaffold for the Treatment of Full-Thickness Chondral Defects of the Knee in Pa-tients Older than 45 Years. Knee Surg Sports Traumatol Arthrosc 2017, 25, 2494-2501, doi:10.1007/S00167-016-3984-6.
https://doi.org/10.1007/s00167-016-3984-6 |
| 100 | Goldring, M.B.; Marcu, K.B. Cartilage Homeostasis in Health and Rheumatic Diseases. Arthritis Res Ther 2009, 11, doi:10.1186/AR2592.
https://doi.org/10.1186/ar2592 |
| 101 | Widuchowski, W.; Widuchowski, J.; Trzaska, T. Articular Cartilage Defects: Study of 25, 124 Knee Arthroscopies. Knee 2007, 14, 177-182, doi:10.1016/J.KNEE.2007.02.001.
https://doi.org/10.1016/j.knee.2007.02.001 |
| 102 | Curl, W.W.; Krome, J.; Gordon, E.S.; Rushing, J.; Smith, B.P.; Poehling, G.G. Cartilage Injuries: A Review of 31, 516 Knee Arthroscopies. Arthroscopy 1997, 13, 456-460, doi:10.1016/S0749-8063(97)90124-9.
https://doi.org/10.1016/S0749-8063(97)90124-9 |
| 103 | Scotti, C.; Gobbi, A.; Karnatzikos, G.; Martin, I.; Shimomura, K.; Lane, J.G.; Peretti, G.M.; Nakamura, N. Cartilage Repair in the Inflamed Joint: Considerations for Biological Augmentation Toward Tissue Regeneration. Tissue Eng Part B Rev 2016, 22, 149-159, doi:10.1089/TEN.TEB.2015.0297.
https://doi.org/10.1089/ten.teb.2015.0297 |
| 104 | Barbero, A.; Grogan, S.; Schäfer, D.; Heberer, M.; Mainil-Varlet, P.; Martin, I. Age Related Changes in Human Articular Chondrocyte Yield, Proliferation and Post-Expansion Chondrogenic Capacity. Osteoarthritis Cartilage 2004, 12, 476-484, doi:10.1016/j.joca.2004.02.010.
https://doi.org/10.1016/j.joca.2004.02.010 |
| 105 | Steadman, J.R.; Briggs, K.K.; Rodrigo, J.J.; Kocher, M.S.; Gill, T.J.; Rodkey, W.G. Outcomes of Microfracture for Traumat-ic Chondral Defects of the Knee: Average 11-Year Follow-Up. Arthroscopy: The Journal of Arthroscopic & Related Surgery 2003, 19, 477-484, doi:10.1053/JARS.2003.50112.
https://doi.org/10.1053/jars.2003.50112 |
| 106 | Mithoefer, K.; Williams, R.J.; Warren, R.F.; Potter, H.G.; Spock, C.R.; Jones, E.C.; Wickiewicz, T.L.; Marx, R.G. The Micro-fracture Technique for the Treatment of Articular Cartilage Lesions in the Knee. A Prospective Cohort Study. J Bone Joint Surg Am 2005, 87, 1911-1920, doi:10.2106/JBJS.D.02846.
https://doi.org/10.2106/JBJS.D.02846 |
| 107 | Knutsen, G.; Isaksen, V.; Johansen, O.; Engebretsen, L.; Ludvigsen, T.C.; Drogset, J.O.; Grøntvedt, T.; Solheim, E.; Strand, T.; Roberts, S. Autologous Chondrocyte Implantation Compared with Microfracture in the Knee. A Random-ized Trial. J Bone Joint Surg Am 2004, 86, 455-464, doi:10.2106/00004623-200403000-00001.
https://doi.org/10.2106/00004623-200403000-00001 |
| 108 | Muschler, G.F.; Nitto, H.; Boehm, C.A.; Easley, K.A. Age- and Gender-Related Changes in the Cellularity of Human Bone Marrow and the Prevalence of Osteoblastic Progenitors. Journal of Orthopaedic Research 2001, 19, 117-125, doi:10.1016/S0736-0266(00)00010-3.
https://doi.org/10.1016/S0736-0266(00)00010-3 |
| 109 | Miller, B.S.; Steadman, J.R.; Briggs, K.K.; Rodrigo, J.J.; Rodkey, W.G. Patient Satisfaction and Outcome after Microfrac-ture of the Degenerative Knee. J Knee Surg 2004, 17, 13-17, doi:10.1055/S-0030-1247141/BIB.
https://doi.org/10.1055/s-0030-1247141 |
| 110 | Gobbi, A.; Karnatzikos, G.; Kumar, A. Long-Term Results after Microfracture Treatment for Full-Thickness Knee Chondral Lesions in Athletes. Knee Surg Sports Traumatol Arthrosc 2014, 22, 1986-1996, doi:10.1007/S00167-013-2676-8.
https://doi.org/10.1007/s00167-013-2676-8 |
| 111 | Abbas, M.; Alkaff, M.; Jilani, A.; Alsehli, H.; Damiati, L.; Kotb, M.; Abdelwahed, M.; Alghamdi, F.; Kalamegam, G. Combi-nation of Mesenchymal Stem Cells, Cartilage Pellet and Bioscaffold Supported Cartilage Regeneration of a Full Thickness Articular Surface Defect in Rabbits. Tissue Eng Regen Med 2018, 15, 661-671, doi:10.1007/S13770-018-0131-0/METRICS.
https://doi.org/10.1007/s13770-018-0131-0 |
| 112 | Aytekin, K.; Esenyel, C.Z. Comparing BST-CarGel® with Hyalofast for the Treatment of Hyaline Cartilage Defects. Euro-pean Archives of Medical Research 2021, 37, 217-222, doi:10.4274/EAMR.GALENOS.2020.76983.
https://doi.org/10.4274/eamr.galenos.2020.76983 |
| 113 | Buda, R.; Vannini, F.; Cavallo, M.; Grigolo, B.; Cenacchi, A.; Giannini, S. Osteochondral Lesions of the Knee: A New One-Step Repair Technique with Bone-Marrow-Derived Cells. J Bone Joint Surg Am 2010, 92 Suppl 2, 2-11, doi:10.2106/JBJS.J.00813.
https://doi.org/10.2106/JBJS.J.00813 |
| 114 | Chen Chou, A.C.; Tjoen Lie, D.T. Clinical Outcomes of an All-Arthroscopic Technique for Single-Stage Autologous Matrix-Induced Chondrogenesis in the Treatment of Articular Cartilage Lesions of the Knee. Arthrosc Sports Med Rehabil 2020, 2, e353-e359, doi:10.1016/j.asmr.2020.05.006.
https://doi.org/10.1016/j.asmr.2020.05.006 |