Original Article - DOI:10.33594/000000727
Accepted 28 Augugst 2024 - Published online 14 September 2024
Analysis of Erythrocyte Parameters in Multiple and Long-Term Blood Donors from Northern Pomerania (Poland)
bJohn Paul II Regional Blood Donation and Treatment Centre in Słupsk, Słupsk, Poland,
cNicolaus Copernicus University in Toruń, Collegium Medicum in Bydgoszcz, Department of Medical Biology and Biochemistry, Department of Ecology and Environmental Protection, M. Skłodowska-Curie St. 9, PL 85-094 Bydgoszcz, Poland,
dUniversity of Zielona Góra, Faculty of Biological Sciences, Institute of Biological Sciences, Department of Biotechnology, Prof. Z. Szafran St. 1, PL 65-516 Zielona Góra, Poland
Keywords
Abstract
Background/Aims:
Assessment of the levels of vital blood parameters in donors is essential to evaluate their health status, ensure their suitability for donation, preserve the integrity of the circulatory system, and facilitate comprehensive health monitoring. The aim of our study was to analyse the levels of haemoglobin, haematocrit, erythrocyte count, MCV, MCH, and MCHC in 12 groups of first-time donors and experienced donors of both sexes at the John Paul II Regional Blood Donation and Treatment Centre in Słupsk, northern Poland. The donors were divided into three age groups (18-30 years, 31-45 years, and 46-65 years).Methods:
Using MANOVA multivariate significance tests, we examined the main effects of donor-related factors (age, sex, donor stage) on morphological blood parameters to evaluate different haematological parameters, such as Hb, Ht, RBC, MCV, MCH, and MCHC, and identified statistically significant relationships between all variables.Results:
The multivariate analysis of these three main factors showed that the variation in haemoglobin (Hb) levels accounted for 46% of the explained dependence in this statistical model. In particular, approximately half of the variability in the multivariate statistical analysis was attributed to the role of Hb and haematocrit (Ht). In addition, the β-coefficient values for Hb and Ht were statistically higher in relation to donor sex and donor type (single versus repeat). These β-coefficient values from our data represent the strength and direction of the relationship between the haematological parameters (Hb and Ht) and the specific donor characteristics. A higher β-coefficient indicates a stronger influence of donor sex and donor type on these parameters, suggesting that these factors contribute significantly to the variation in the Hb and Ht levels. Based on our results, the comprehensive analysis of the entire statistical model of metabolic biomarkers revealed the following hierarchy: Hb > Ht > MCHC > MCV > RBC > MCH. The results obtained showed strong statistical relationships, as indicated by the high values of the key statistical indicators in our analysis. The coefficient of determination (R²) showed that the model explained a significant proportion of the variance in the data, while the F-test statistic confirmed the significance of the predictors.Conclusion:
These strong statistical dependencies provided a clear justification for selecting this model over others, as it effectively represented the underlying relationships within the data. These statistics help to assess how well the model matches the actual data, thereby helping to reduce the risks associated with blood donation, optimise donor safety, and maintain the quality and efficiency of blood transfusion services.Introduction
Blood donation is a vital aspect of healthcare that relies on the generosity of donors to maintain an adequate blood supply for transfusion and medical treatment (1). Multiple and long-term blood donors play a crucial role in this process, often exhibiting unique characteristics in their red cell parameters due to their frequent donation practices (2). Our study is a first step in examining this issue on a large scale. By examining a large dataset, we aim to lay the baseline for further investigations into the unique characteristics observed in long-term blood donors. The unique characteristics observed in multiple and long-term blood donors - such as different erythrocyte parameters and variations in haemoglobin levels - are interesting but remain poorly understood from a genetic and immunological perspective as well as in relation to such factors as iron metabolism (3-8), diet (9, 10), lifestyle (11, 12) and psycho-emotional state (13). Although these characteristics are known, there is a notable gap in understanding the responses that contribute to long-term adaptation in blood donors and the impact of the interactions between haematological balances and metabolic processes on these parameters. Further research in these areas is needed to fully elucidate the underlying mechanisms and implications of these unique donor profiles.
Blood donation is a cornerstone of modern healthcare systems worldwide (14). It plays a pivotal role in ensuring the availability of vital blood components needed for various medical procedures, including surgery, treatment of chronic diseases, trauma care, and emergencies. Donated blood and its components, such as red cells, platelets, and plasma, are essential resources that save millions of lives every year. One of the main purposes of blood donation is to replenish blood supplies in blood banks and hospitals (15, 16). These supplies are in constant demand to meet the needs of patients suffering from such conditions as cancer, anaemia, bleeding disorders, and obstetric complications. Without an adequate and consistent supply of donated blood, healthcare providers would struggle to perform critical medical interventions and surgeries, putting patients’ lives at risk (17). Encouraging and facilitating blood donation is therefore essential to protect the health and well-being of individuals and communities worldwide (18-22).
Multiple and long-term donors are individuals who have made numerous donations over an extended period of time, demonstrating a strong commitment to blood donation (23-25). These donors play a critical role in maintaining the blood supply, often serving as a reliable source of blood products for hospitals and healthcare facilities (24). Multiple donors typically give blood regularly, sometimes exceeding the average frequency of donation recommended for the general population (14). Their consistent donations make a significant contribution to maintaining an adequate blood supply, particularly during periods of increased demand or shortage. Although the influence of individual and contextual factors on donor status and behaviour is well established, the underlying mechanisms remain poorly understood. Piersma et al. (26) highlighted the importance of longitudinal studies focusing on donor behaviour, in particular examining the impact of life events and network dynamics on blood donor careers. Therefore, a better understanding of donor behaviour will help policy makers in blood collection organisations to ensure a consistent and adequate blood supply, which is paramount. This is because multiple and long-term donors may have unique characteristics in their donation profiles and physiological parameters compared to occasional or first-time donors. Studying these characteristics can provide insights into the impact of repeated blood donation on donor health and well-being and identify potential strategies to support the long-term health of these dedicated individuals (26).
Iron plays a crucial role in the health and well-being of blood donors, directly influencing the quality of donated blood (27). Therefore, the importance of iron levels in blood donors is a topic that is actively debated in the literature. Iron is indeed a critical factor for blood donors, as it is directly linked to haemoglobin levels, affecting the quality of donated blood and the donor’s overall health (28, 7). It is known that haemoglobin, i.e. the protein in red blood cells responsible for the transport of oxygen, is dependent on adequate iron levels to maintain its functionality (29). However, iron is only one of several key factors that influence blood donation. Other factors are also important: overall health and nutrition, including vitamins B12 and folate, are essential for red blood cell production (30, 31), hydration levels are important to maintain blood volume and prevent dehydration (32), and the frequency of donation affects the donor’s ability to replenish blood components and iron stores (33). In addition, psycho-emotional well-being and hormonal balance can affect both donor health and blood quality (9, 34). The importance of iron levels in blood donors is a topic that is actively debated in the literature (35-37). Adequate iron levels are essential to maintain haemoglobin levels, which are critical for oxygen transport in the body (29). However, repeated blood donations can lead to depletion of iron stores in donors, potentially resulting in iron deficiency and anaemia (35). Therefore, regular monitoring of iron levels in blood donors and appropriate interventions, such as iron supplementation or deferral of donation, are essential to prevent adverse health outcomes and ensure the safety of both donors and recipients. In addition, strategies to optimise iron repletion and minimise iron loss through dietary interventions and donation management are being actively explored to protect donor health and the sustainability of blood donation programmes (38-40).
The issue of fundamental differences between men and women in blood donation and the blood from one-time and repeat donors is poorly understood and requires further research. This is due to several factors, including the complexity of the biological processes involved in blood donation, potential differences in the response to donation stressors between men and women, and the need for comprehensive longitudinal studies to thoroughly understand the impact of repeated donations on blood parameters (41, 42). The influence of such factors as age (43), hormonal status (44), and lifestyle habits (13) on blood parameters highlights the need for further research in these areas. Furthermore, donor demographics, frequency of donation, and duration of donation history will be considered in the analysis to provide a comprehensive understanding of the relationship between blood donation frequency and red cell parameters (26). The results of a similar study will provide valuable insights for blood donation programmes, helping to develop tailored strategies to support the health and well-being of multiple and long-term blood donors, while ensuring the sustainability of blood donation services.
Our study, conducted at the John Paul II Regional Blood Donation and Treatment Centre in Słupsk (northern Poland), aimed to analyse: i) the erythrocyte parameters in individuals who had donated blood once and those who had been long-term blood donors in different age groups (18-30 years, 31-45 years, and 46-65 years), including both sexes. This analysis aimed to identify any significant trends or differences compared with occasional or first-time donors. ii) By examining key parameters including haemoglobin levels, haematocrit, red blood cell (RBC) count, mean corpuscular volume (MCV), mean corpuscular haemoglobin (MCH), and mean corpuscular haemoglobin concentration (MCHC), our research aimed to elucidate the potential impact of repeated blood donation on the physiological status of donors; iii) In addition, our study used the multivariate analysis of variance (MANOVA) supported by the results of the sum-of-squares test (total SS model vs. residual SS), as well as multiple correlation analysis (R), coefficient of determination (R2), and its corrected form adjusted for random error (R2 adjusted). Through these analytical approaches, we aimed to gain a comprehensive understanding of the relationship between blood donation frequency and erythrocyte parameters.
Materials and Methods
Ethical approval
The experiments were conducted by the Guidelines of the European Union Council and the current laws in Poland. The study was conducted with the statement on bioethical approval of the Bioethics Committee of Gdansk (KB 41/23). All studies involving human blood were approved by the institutional review board of the Bioethical Commission at Gdańsk Medical University (No KB-41/23, 9.10.2023).
Experimental design
The research was conducted at the John Paul II Regional Blood Donation and Treatment Centre in Słupsk (northern Poland), which operates as an independent unit in 3 field branches. We analysed results obtained from healthy voluntary donors aged 18-65 years. Blood was analysed after collection from donors of different age and sex divided according to the characteristics of blood donation frequency: 1) first-time donors - those who donate blood for the first time and 2) multiple donors - those who systematically donate blood at least twice within 24 months (according to the blood transfusion service in Poland), as shown in another study (45). Blood was collected both at the headquarters of the John Paul II Regional Blood Donation and Treatment Centre in Słupsk and at two field branches in Chojnice and Lębork (Pomeranian Voivodeship, Poland). The blood donation was carried out with the help of mobile blood collection teams in the whole area of operation of the Regional Blood Donation and Blood Treatment Centre, i.e. in the districts of Bytów, Chojnice, Człuchów, Lębork, Słupsk, and the city of Słupsk with the rights of a district, mainly through a mobile blood collection unit.
Fig. 1: Study design.
Characteristics of blood donors
Blood samples were taken from healthy individuals aged between 18 and 60 years (up to 65 years with medical consent). In Poland (as in many European countries), the permissible frequency of whole blood donations per year is 6 times for men and 4 times for women, with an interval of at least 8 weeks. In addition, a complete blood count is performed once a year for each donor. A first-time donor is defined as a person who has not previously donated blood for therapeutic purposes and a repeat donor is defined as a donor who donates blood regularly (at least twice in the last 24 months).
Prior to each donation, the donor’s laboratory results are reviewed by a qualified physician, a donor questionnaire that includes detailed questions about the donor’s past and present health and possible risk behaviours is completed and a physical examination (abbreviated physical and subject examination) is performed. The test to qualify for blood donation is the haemoglobin (Hb) level, which is determined in blood taken from the finger. In Poland, the Hb level of ≥12.5 g/dl for women and ≥13.5 g/dl for men is required to qualify a donor to give blood (46); the same values are used in some European countries. In the USA and Canada, however, donors can give whole blood every 56 days if their Hb concentration is at least 13 g/dl (men) and 12.5 g/dl (women), as shown in another study (47).
Typically, 450 ml of whole blood is collected from each donor. Blood is collected in sterile disposable aphaeresis container sets made of plastic materials, integrally connected and containing aphaeresis preservative fluid (Citrate–phosphate–dextrose (CPD) solution 63 ml, citric acid monohydrate 3, 27 g, sodium citrate dihydrate 26, 3 g, sodium dihydrogen phosphate monohydrate 2, 51 g, glucose monohydrate 25, 5 g, aqua for injection, up to 1000 ml). One unit of whole blood collected is 450 ml ± 10% mixed with preservative fluid.
For each collected donation, blood samples are taken for a number of tests, including markers of infectious factors: syphilis test, HBs antigen, anti-HCV antibodies, and anti-HIV 1/2 antibodies as well as HCV RNA, HBV DNA, and HIV RNA. Blood grouping within the ABO, RhD, and K systems and antibody screening are performed for each collected donation (48, 49).
Blood donor groups analyse
All the blood donors were divided into 12 groups based on the frequency of donation (disposable, multiple), gender (female, male), and three age groups (18-30, 31-45, and 46-65 years), totalling 700 individuals. The blood donors were divided into one-time donors, age group 18-30 years, 450 ml of blood (disposable, one-time or first blood donation, DBD, n = 50), one-time donors, age group 31-45 years, 450 ml of blood (DBD, n = 75), one-time donors, age group 46-65 years, 450 ml of blood (DBD, n = 50); long-term regular blood donors (LRBD, n = 50), long-term regular blood donors (LRBD, n = 75), 31-45 years, 1-15 litres, and 46-65 years, 2-15 litres; in the case of men, the blood volume was 450 ml in the age group 18-30 years (DBD, n = 50) and in the age groups 31-45 years (DBD, n = 75) and 46-65 years (DBD, n = 50); in the group of long-term regular blood donors, the blood volume was 2-12 litres at 18-30 years (LRBD, n = 50), 2-20 litres at 31-45 years (LRBD, n = 75), and 1-55 litres at 46-65 years (LRBD, n = 50).
Sample collection for analysis
Disposable equipment was used to collect material for analyses. Blood samples were collected in tubes using a closed vacuum system. Specifically, venous blood samples were collected in 2-ml tubes containing K3-EDTA anticoagulant to maintain stability for 24 hours at temperatures in the range of 2-8°C. K3-EDTA maintains good sample stability and prevents clotting. It also helps to inhibit glycolysis, preserving the integrity of blood samples, and has no effect on the MCV of red blood cells at higher concentrations. Prior to the analysis, the samples were mixed on a haematological mixer (Universal Hematology Mixer, TYPE UMH-5, WIGO, Poland) for 5 minutes.
Determination of red blood cell morphology
Determination of erythrocyte morphology was performed using a SYSMEX XN-550 haematology analyser (SYSMEX, Poland), i.e. an automated 5-part differential analyser with a sample aspiration volume of 25µl. The SYSMEX XN-550 analyser includes fluorescence flow cytometry, hydrodynamic focusing, and the cyanide-free SLS method for haemoglobin determination.
Our analyses were performed using the SYSMEX XN-550 haematology analyser. This equipment uses fluorescence flow cytometry to measure erythrocyte morphology, providing data on cell volume, internal structures, and nucleic acid content. The presence of cells or particles in the path of the laser beam results in the generation of three distinct signals: forward scatter, side scatter, and side fluorescence light. The intensity of the forward scatter indicates the cell volume. The side scatter provides information about the interior of the cell, such as the nucleus and granules. The amount of DNA and RNA present in the cell is indicated by side fluorescence. The SYSMEX analyser uses a sheath liquid and a direct current detection method to count red blood cells (RBCs) in million blood cells/μl. We used this analyser to count red blood cells (RBCs) by impedance with hydrodynamic focusing and to measure the haemoglobin concentration with a cyanide-free photometric method with sodium lauryl sulphate (SLS). The hydrophilic groups of SLS molecules bind to the haeme group, forming a stable-coloured complex (SLS-HGB), which is analysed using a photometric method. A LED diode emits monochromatic light, which passes through the mixture and is absorbed by SLS-HGB complexes. The absorbance, measured by a photoelectric sensor, is proportional to the concentration of haemoglobin in the sample.
In our study, we found no significant changes in Hb and Ht levels, and the blood donors did not report any discomfort during medical interviews. Therefore, additional analysis of iron levels was not considered necessary, as there was no evidence of iron deficiency or adverse effects associated with blood donation.
Statistical analysis
The statistical analysis was performed using the Statistica 13.3 package (TIBCO Software, Palo Alto, CA, USA). Analysis results were expressed as mean ± standard deviation. A multiple range test was used to determine significant differences between means, with P values < 0.05 considered statistically significant. Prior to the analysis, data were assessed for homogeneity of variance using Levene’s test and for normality using the Kolmogorov-Smirnov test. Three-way ANOVA and Tukey’s post-hoc test were used to analyse differences between values obtained for all donor groups based on the stage, age, and sex. The use of multivariate significance tests allowed us to examine the main effects (age, sex, donor stage) on morphological blood parameters commonly assessed in studies evaluating different haematological parameters, such as Hb, Ht, RBC, MCV, MCH, and MCHC, and to identify statistically significant relationships for all variables. The model included the main effect of their interaction as well as the experimental random error assessed by the F-test and its significance.
In addition, the multivariate analysis of variance (MANOVA) was supported by sum-of-squares test results (total SS model vs. residual SS) for multiple correlation analysis (R), coefficient of determination (R2), and its corrected form adjusted for random error in data analysis (R2 adjusted). The coefficient of determination serves as the primary indicator of the quality of the regression model and describes the relationship between dependent and independent variables in the statistical model.
Standardised β-coefficients of regression were used to assess multivariate dependencies and the influence of the analysed predictors in the model of blood donor age, sex, and frequency criteria. This made it possible to compare the overall effect of each predictor on the dependent variable with the effect of other predictors and to assess the combined effects of the main factors on each of the morphological parameters of the red blood cells studied in the blood of donors (50).
Results
Haemoglobin levels in one-time and long-term blood donors according to sex and age
We used the multivariate tests of significance with σ-restricted parameterization and effective hypothesis decomposition in the statistical analysis to analyse the role of the following main factors: sex of disposable (DBD) and long-term regular (LRBD) blood donors, multiplex, and age of blood donor groups (18-30 years, 31-45 years, and 46-65 years). The regression analysis of the haemoglobin (Hb, g/dl) data in all the groups for the main effect of sex showed a statistically significant t-test value of 24.16 (p = 0.000). The result of the analysis of variance was F3.698 = 199.32 and was also statistically significant. The summary results of the regression analysis were as follows: R = 0.692 and the coefficient of determination for Hb the in these conditions was R2 = 0.461 and R2adj = 0.459. Thus, the analysis of the multivariate variation for the Hb parameter corresponds to the value of 46% of the dependence explanation in this statistical model, i.e. half of the variability in the multivariate statistical analysis was determined by the role of Hb.
The analysis of the value of the β-coefficient, which determines the unified role of the main factor in the variability of the Hb parameter in the statistical analysis, was β = 0.706 ± 0.029 for the donor sex and β = -0.29 ± 0.29 for the multiple donor type, which indicates a higher dependence of the Hb level on the sex than on the multiple donor type. Both values were statistically significant. A detailed description of these data is shown in Table 1.
It should be noted that the values of all Hb levels for this data set were within the normal range for the age and sex of the patients according to the criteria for donation in Poland (45, 46, 51). It is important to note that the values of Hb in our studies showed the highest values in the group of women aged 31-45 years and the lowest in this group of multiple donors aged 18-30 years; in the group of men, the highest Hb values were in the group of younger men aged 18-30 years who were beginning their blood donation experience and the lowest in the older donors aged 46-65 years with a long history of donation. In our study of Hb levels, the mode value, which is characterised as one or more values in a set of observations that occur most frequently and show the typicality of the observation value, was 13.9 and was recorded in this population in five patients, with a median value of 14.3. These data are also presented in Table 1. In the case of the Hb data, the lower and upper quartiles of the experimental data sample, the median of the lower half of the sample, and the median of the upper half of the sample, respectively, are given, as well as variation values showing differences in haemoglobin level values in relation to age, type of the donation process (first-time donors), and in blood donors of different ages.
This table also shows the values of the coefficient of variability, which indicates the degree of variability with respect to the sample mean and is expressed as a percentage. We obtained statistically significant differences between the groups by sex, i.e. male and female donors in their age groups, and by the type of the blood donation process (primary or regular multiple donation). It is important to note that the variability process specification showed the lowest values for the indicators for the female group (LRBD, age 18-30, n = 50) and the highest for this sample for the male group (LRBD, age 46-65, n = 50). Skewness characterises the degree of asymmetry of the data distribution around its mean, and the results of our observations show low values of this parameter, which may indicate a low degree of differences when comparing the distribution of the analysed Hb variable with a hypothetical normal distribution.
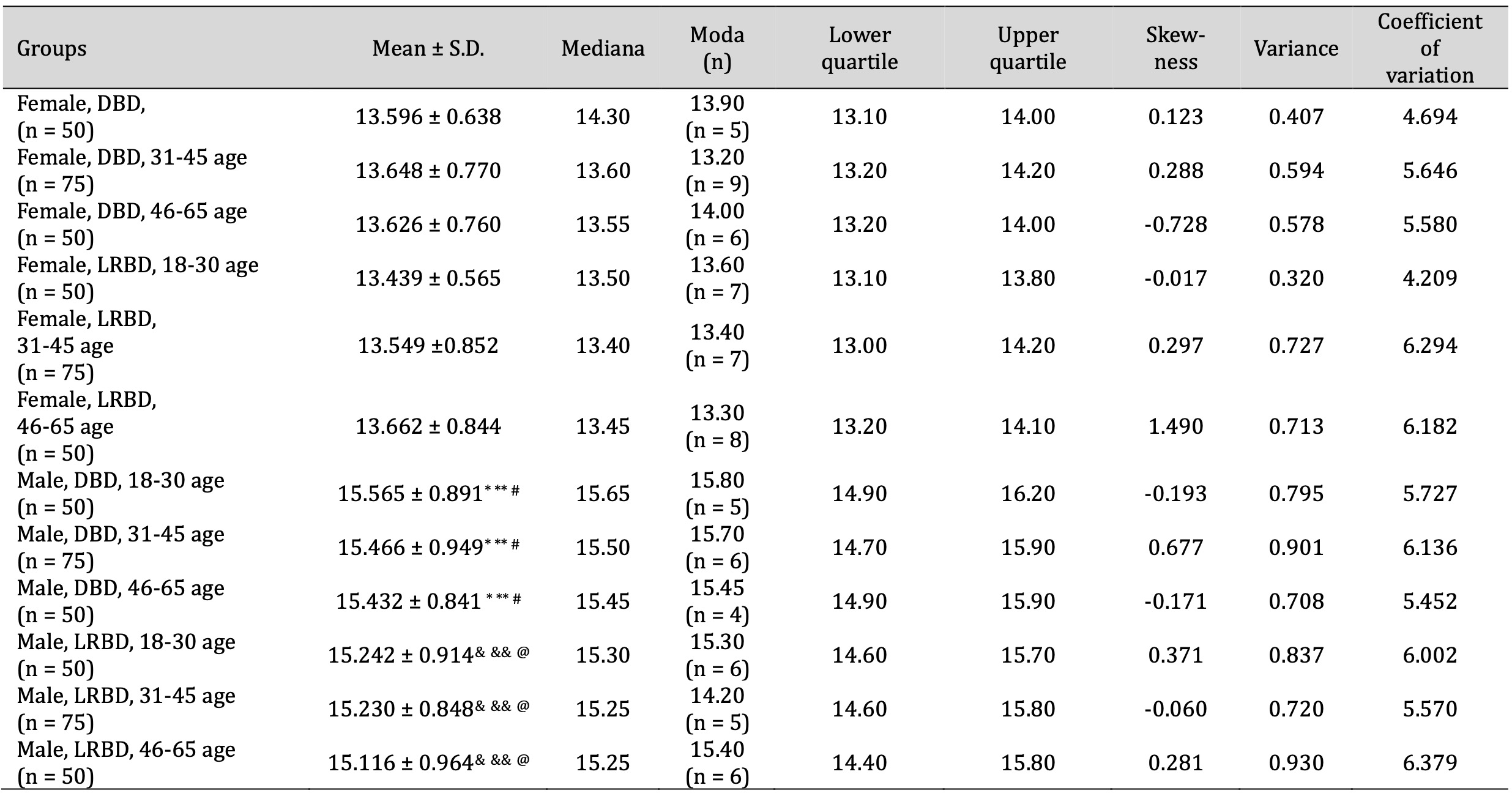
Table 1: Haemoglobin level (g/dl) in disposable blood donors (DBD) and long-term regular blood donors (LRBD) by sex and age. ANOVA post-hoc analysis with Tukey’s HSD test between the groups. * Significant changes between groups: female, DBD or LRBD, 18-30 years and male, DBD, 18-30 years at p < 0.05; ** Significant changes between groups: female, DBD or LRBD, 31-45 years and male, DBD, 31-45 years at p < 0.05; # Significant changes between groups: female, DBD or LRBD, age 46-65 and male, DBD, age 46-65 at p < 0.05;& Significant changes between groups: female, DBD or LRBD, 18-30 years and male, LRBD, 18-30 years at p < 0.05;&& Significant changes between groups: female, LRBD, age 31-45 and male, LRBD, age 31-45 at p < 0.05;@ Significant changes between groups: female, LRBD, age 46-65 and male, LRBD, age 46-65 at p < 0.05
Haematocrit value
As haematocrit (Ht) is a key parameter in understanding the health and oxygen-carrying capacity of the blood, this was the next stage of our study. Ht indicates the proportion of red blood cells in blood, expressed as a percentage, and depends on the number and size of red blood cells. The normal Ht range is 40.7-50.3% for males and 36.1-44.3% for females. Our data confirm these levels of distribution of the parameters in the donor groups studied.
The regression analysis of the dependent variable according to the Ht parameter performed using MANOVA correlation coefficient analysis showed the value R = 0.639. For the coefficient of determination in the linear regression model analysed here, this coefficient indicates the proportion of variance in the dependent variable (Ht) associated with the predictor (independent) values, such as gender and multiple donations, at the level of R2 = 0.409. The statistical analysis also shows the use of the corrected value of the coefficient, which is useful in the model selection process, as it helps to identify models that effectively explain the variance in the dependent variable without introducing unnecessary complexity and is used in the corrected form as R2adj = 0.407.
The F coefficient showed a Ht value of F3.698 = 161.26, which was statistically significant. The standardised beta regression coefficient showed the following values for the Ht parameter: β = 0.670 ± 0.031 for the gender factor and slightly smaller for the multiple donation factor with β = -0.234 ± 0.030. These relationships were statistically significant for the above factors (predictors).
The data on Ht values for all the donors in the study group are presented in Table 2. As analysed previously, these changes were statistically significant for the donor groups of different sexes and similar to the statistically significant relationships presented previously for Hb, as these parameters are significantly correlated in the determination and analysis of blood. The highest Ht values were found in the group of the female donors LRBD (31-45 years) and the lowest in the DBD group (18-30 years). In the male donor group, the highest Ht values were found in the DBD group (18-30 years) and the lowest in the LRBD group (18-30 years).
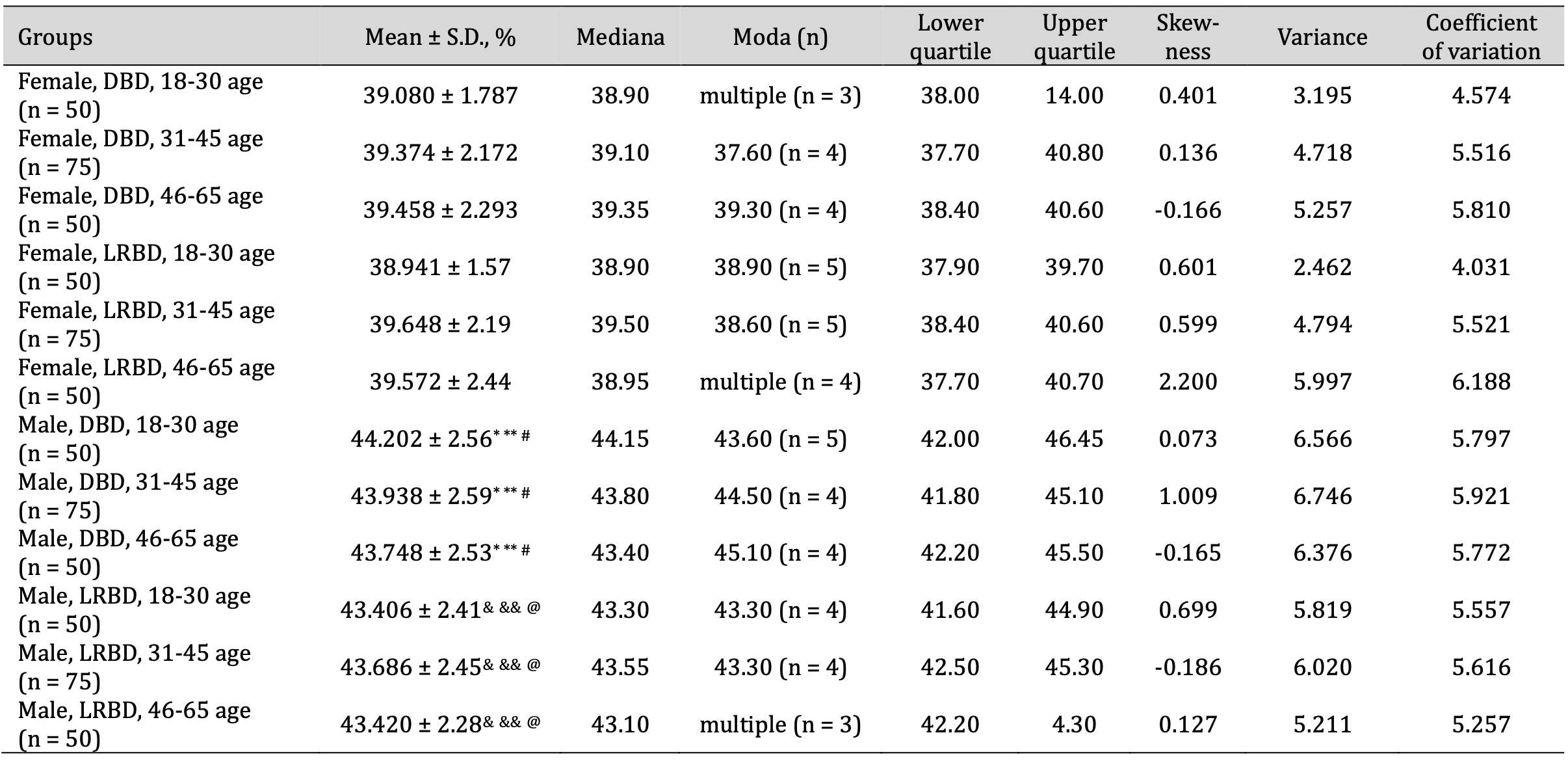
Table 2: Haematocrit level (%) in disposable blood donors (DBD) and long-term regular blood donors (LRBD) by sex and age. ANOVA post-hoc analysis with Tukey’s HSD test between the groups. * Significant changes between groups: female, DBD or LRBD, 18-30 years and male, DBD, 18-30 years at p < 0.05; ** Significant changes between groups: female, DBD or LRBD, 31-45 years and male, DBD, 31-45 years at p < 0.05; # Significant changes between groups: female, DBD or LRBD, age 46-65 and male, DBD, age 46-65 at p < 0.05;& Significant changes between groups: female, DBD or LRBD, 18-30 years and male, LRBD, 18-30 years at p < 0.05;&& Significant changes between groups: female, LRBD, age 31-45 and male, LRBD, age 31-45 at p < 0.05;@ Significant changes between groups: female, LRBD, age 46-65 and male, LRBD, age 46-65 at p < 0.05
RBC value
The results of the regression analysis of the dependent variables relative to the WBC parameter corresponded to the following values: R = 0.130, R2 = 0.017, and R2adj = 0.013 at F3.698 = 4.039 and was statistically significant. The standardised β regression coefficient was β = 0.133 ± 0.039 and was the lowest, as observed from the previous data analysis. The data on erythrocyte values for all donors in the study group are shown in Table 3. The use of MANOVA for this analysis, followed by Tukey’s post-hoc tests for uneven data, showed no differences between our study RBC counts in all the donor groups studied and showed no dependence on sex or multiple donation. In the group of female donors, the minimum RBC values were observed in the LRBD group (18-30 years) and the maximum in the LRBD group (46-65 years). It is important to note that, in this case, the maximum values of the RBC level in the female LRBD group were also associated with the highest value of variation and, accordingly, with the highest coefficient of variation among the data examined in the statistical analysis (Table 3).
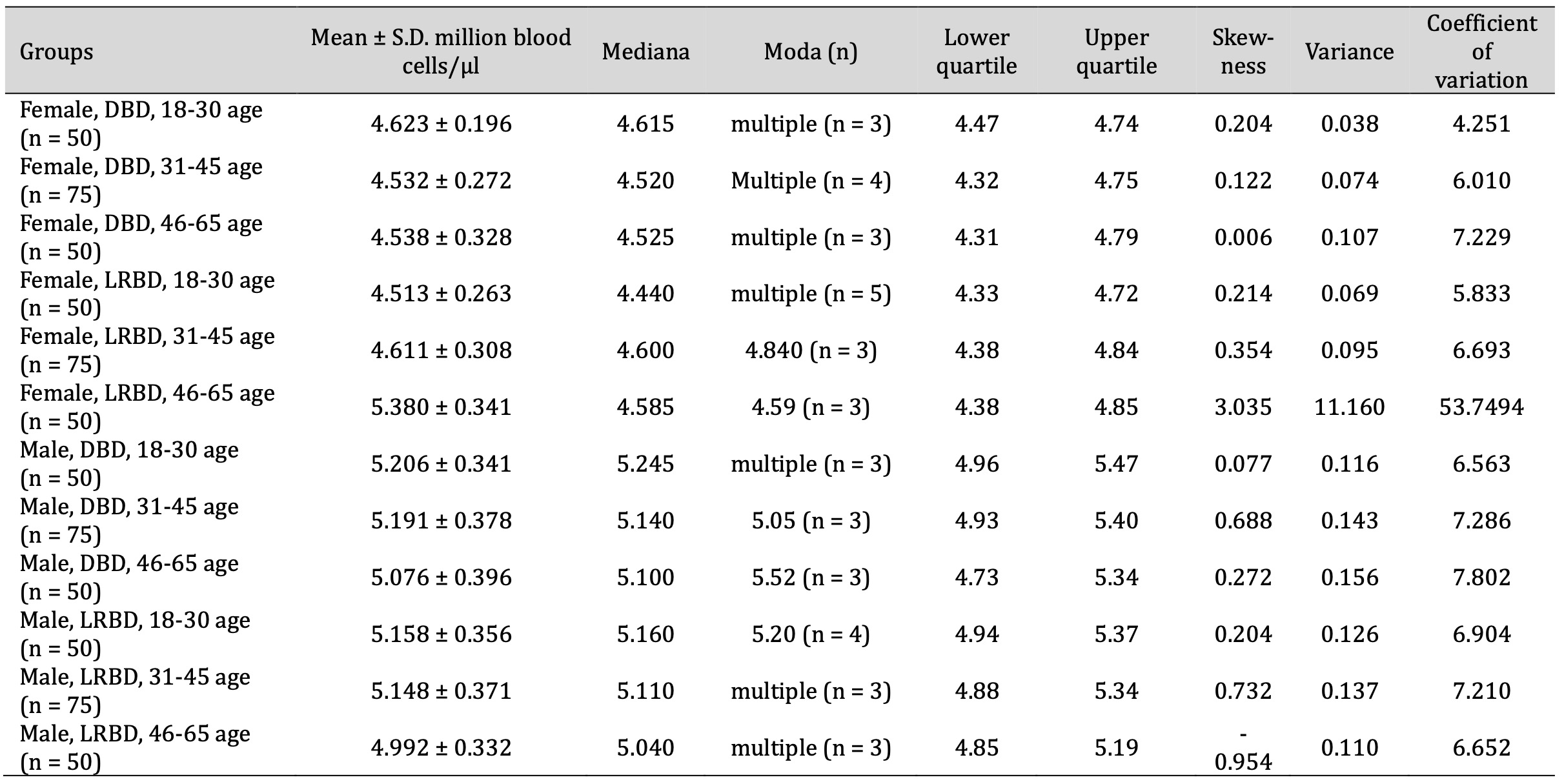
Table 3: RBC count (million blood cells/μl) in disposable blood donors (DBD) and long-term regular blood donors (LRBD) according to sex and age. ANOVA post-hoc analysis with Tukey’s HSD test between the groups. * Significant changes between groups: female, DBD or LRBD, 18-30 years and male, DBD, 18 -30 years at p < 0.05; ** Significant changes between groups: female, DBD or LRBD, 31-45 years and male, DBD, 31-45 years at p < 0.05; # Significant changes between groups: female, DBD or LRBD, age 46-65 and male, DBD, age 46-65 at p < 0.05;& Significant changes between groups: female, DBD or LRBD, 18-30 years and male, LRBD, 18-30 years at p < 0.05;&& Significant changes between groups: female, LRBD, age 31-45 and male, LRBD, age 31-45 at p < 0.05;@ Significant changes between groups: female, LRBD, age 46-65 and male, LRBD, age 46-65 at p < 0.05
MCH, MCHC, and MCV value
MCH, MCHC, and MCV are important parameters measured in a complete blood count that provide valuable information about the size and Hb content of red blood cells. MCH expressed in picograms (pg) per cell, MCHC in grams per decilitre (g/dL), and MCV in femtoliters (fL). In multiple donors, monitoring these values is critical for assessment of the overall health of their blood cells and to detect any potential abnormalities or deficiencies, as shown in Tables 4-6.
The maximum MCH value was recorded in the female DBD group aged 31-45 years, and in the DBD group aged 46-65 years, while the minimum value was determined in the DBD group aged 18-30 years. In the male group, the maximum and minimum MCH values were found in DBD aged 31-45 years and LRBD aged 18-30 years, respectively. There were no statistically significant differences in these MCH values between the study groups (Tab. 4).
The MCHC (Tab. 5) data indicating the concentration of haemoglobin in a given volume of packed red blood cells showed statistical differences in the analysis of variance carried out with the F-test with F11.690 = 5.742 (p = 0.000). Since the regression analysis of the dependent variable showed a statistically significant relationship with the predictor variables, and the key predictors had varying degrees of influence on the dependent variable and contributed to its overall prediction, our research revealed the following relationships for MCHC. We showed a value of β = 0.227 ± 0.038 for donor gender and multiple donor participation, and the corresponding negative value was β = -0.226 ± 0.038. In conclusion, these results provide valuable insights into the factors influencing the dependent variable MCHC and may help in decision making. The data regarding the significance of the regression analysis of the dependent variable according to the MCHC parameter corresponded to R = 0.261, R2 = 0.068, and R2adj = 0.064.
MCV (Mean Corpuscular Volume) measures the average volume or size of red blood cells (Tab. 6). In our study, after the analysis of variance performed with the F-test, the value was F11.690 = 4.058 (p = 0.000). There were statistically significant differences in the MCHC and MCV parameters between the groups of DBD men and women aged 31-45 years. The MANOVA analysis of the MCV data showed a predicted negative value of β = -0.105 ± 0.039 for donor sex, and the main factor analysis showed β = 0.163 ± 0.037 for multiple donor participation. The results of the regression analysis of the dependent variables relative to the MCHC parameter corresponded to the following values R = 0.198, R2 = 0.039, and R2adj = 0.035.
Thus, our regression analysis of the MCH, MCHC, and MCV parameters revealed significant findings in relation to the dependent variables. Importantly, this statistical model accounts for the significant variability in the three dependent variables analysed, with the relationships between predictor variables, such as gender, age, and frequency of donation, collectively contributing to their prediction. We have shown that, unlike the levels of Hb, RBC, and Ht, in this case each predictor variable has a different degree of influence on the dependent variables, some of which have consistent positive or negative associations. The complete analysis of the whole model of statistical dependencies in the biomarkers of metabolic processes showed the following results: Hb > Ht > MCHC > MCV > RBC > MCH. In summary, this statistical model fits well overall and its credibility is enhanced by the various statistics mentioned above. These statistics include various indicators, such as the coefficient of determination (R²), the F-test statistic, and other metrics that help to assess how well the model fits the actual data. The good result of these statistics suggests that the model is appropriate for the data, thereby increasing the credibility of the analysis.
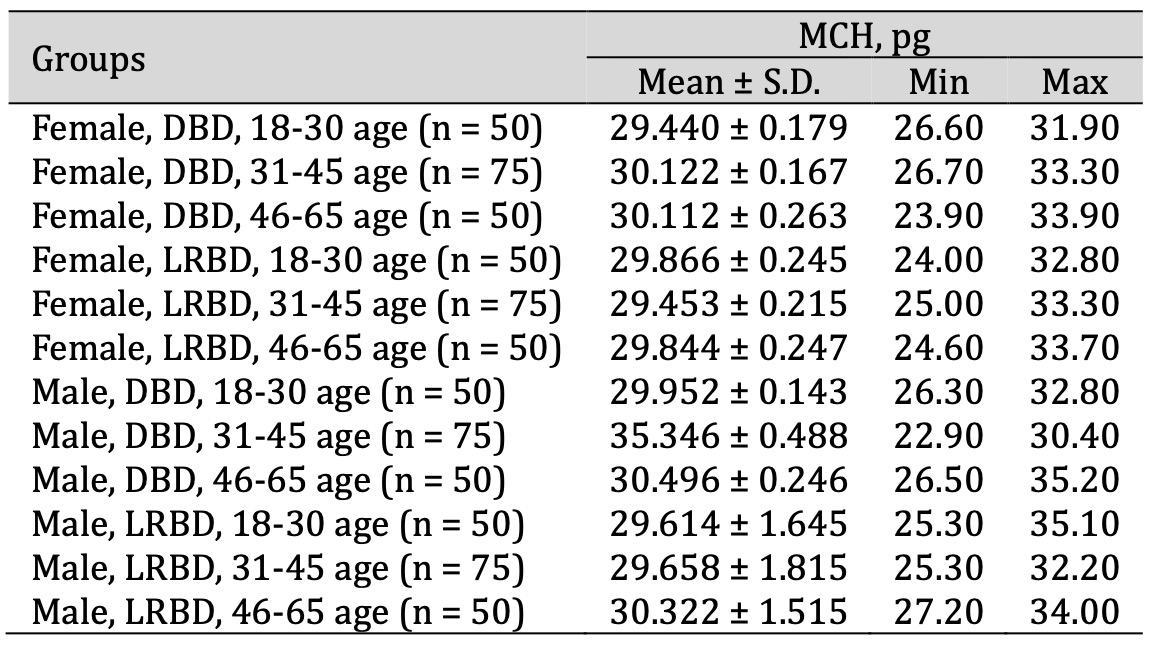
Table 4: MCH (pg) level in disposable blood donors (DBD) and long-term regular blood donors (LRBD) according to sex and age. ANOVA post-hoc analysis with Tukey’s HSD test between the groups. * Significant changes between groups: female, DBD or LRBD, 18-30 years and male, DBD, 18 -30 years at p < 0.05; ** Significant changes between groups: female, DBD or LRBD, 31-45 years and male, DBD, 31-45 years at p < 0.05; # Significant changes between groups: female, DBD or LRBD, age 46-65 and male, DBD, age 46-65 at p < 0.05;& Significant changes between groups: female, DBD or LRBD, 18-30 years and male, LRBD, 18-30 years at p < 0.05; && Significant changes between groups: female, LRBD, age 31-45 and male, LRBD, age 31-45 at p < 0.05;@ Significant changes between groups: female, LRBD, age 46-65 and male, LRBD, age 46-65 at p < 0.05
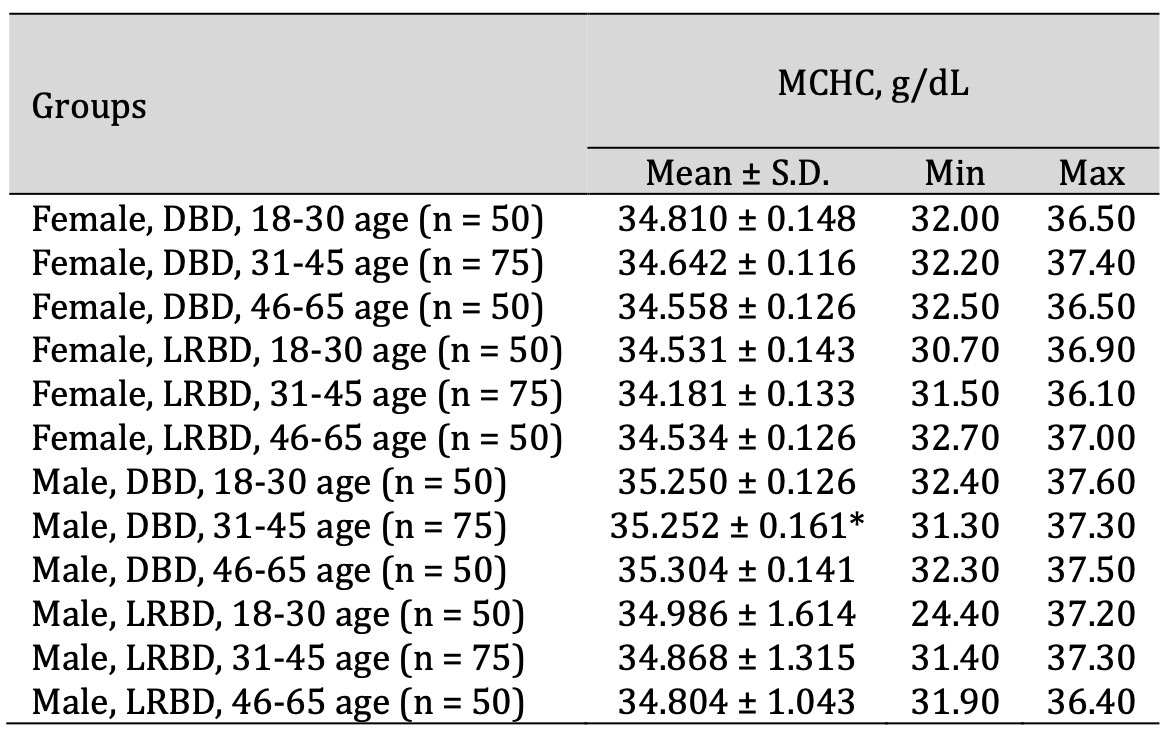
Table 5: MCHC (g/dL) level in disposable blood donors (DBD) and long-term regular blood donors (LRBD) according to sex and age. ANOVA post-hoc analysis with Tukey’s HSD test between the groups.* Significant changes between groups: female, DBD or LRBD, 18-30 years and male, DBD, 18 -30 years at p < 0.05; ** Significant changes between groups: female, DBD or LRBD, 31-45 years and male, DBD, 31-45 years at p < 0.05; # Significant changes between groups: female, DBD or LRBD, age 46-65 and male, DBD, age 46-65 at p < 0.05;& Significant changes between groups: female, DBD or LRBD, 18-30 years and male, LRBD, 18-30 years at p < 0.05;&& Significant changes between groups: female, LRBD, age 31-45 and male, LRBD, age 31-45 at p < 0.05; @ Significant changes between groups: female, LRBD, age 46-65 and male, LRBD, age 46-65 at p < 0.05

Table 6: MCV (fL) level in disposable blood donors (DBD) and long-term regular blood donors (LRBD) according to sex and age. ANOVA post-hoc analysis with Tukey’s HSD test between the groups. * Significant changes between groups: female, DBD or LRBD, 18-30 years and male, DBD, 18 -30 years at p < 0.05; ** Significant changes between groups: female, DBD or LRBD, 31-45 years and male, DBD, 31-45 years at p < 0.05; # Significant changes between groups: female, DBD or LRBD, age 46-65 and male, DBD, age 46-65 at p < 0.05;& Significant changes between groups: female, DBD or LRBD, 18-30 years and male, LRBD, 18-30 years at p < 0.05;&& Significant changes between groups: female, LRBD, age 31-45 and male, LRBD, age 31-45 at p < 0.05; @ Significant changes between groups: female, LRBD, age 46-65 and male, LRBD, age 46-65 at p < 0.05
Discussion
Our research represents a pioneering effort to explore the unique characteristics of multiple and long-term blood donors and their impact on donor health and well-being. By shedding light on these important issues, we aim to improve our understanding of blood donation practices and contribute to the development of effective strategies to support the long-term health of committed blood donors. Long-term donors are individuals who have donated blood for an extended period of time, often years or even decades. These dedicated donors have made blood donation a habitual part of their lives, driven by altruism, compassion, and a desire to make a positive impact on others. The contributions of multiple and long-term blood donors are invaluable to healthcare systems, providing a stable and reliable source of blood products. Their continued support ensures that patients who need transfusions or other blood-related treatments receive timely and appropriate care. Here are the key points in bullet form.
First, we conducted a comprehensive analysis of the unique characteristics exhibited by multiple and long-term blood donors. A comprehensive analysis of the unique characteristics of multiple and long-term blood donors includes several biological factors that contribute to their continued commitment and suitability for regular donation. Studies on this type of blood donors are poorly represented in the literature. They will serve as a basis for exploring other relationships in the fields of biochemistry, immunology, and ecophysiology. A large number of blood samples were analysed in this study and the selection of donors on the basis of gender, age, and frequency of donation will provide a basis for further more extensive research. These findings are only a preliminary part of this wider study. First, physiological adaptations occur in these donors over time, resulting in increased red blood cell production and improved iron metabolism to replace blood lost through donation. Studies have shown that frequent blood donation stimulates erythropoiesis, resulting in higher haemoglobin levels and improved oxygen-carrying capacity in long-term donors.
Our results from the correlative and regression analyses confirm that assessment of Hb levels is essential to evaluate the health status of blood donors, ensure donor eligibility, maintain the integrity of the blood supply, and promote overall health monitoring. By monitoring Hb levels, healthcare professionals can reduce the risks associated with blood donation, optimise donor safety, and maintain the quality and effectiveness of blood transfusion services (52). Our findings in the correlative analysis are confirmed by the summary correlations between Hb-Ht (r = 0.921, p = 0.000), Hb-RBC (r = 0.188, p = 0.000), and Hb-MCH (r = 0.382, p = 0.000).
Hb, a key component of red blood cells, plays a central role in oxygen transport throughout the body. Its primary function is to bind oxygen in the lungs and deliver it to tissues and organs to ensure adequate oxygenation of cells for physiological processes (53). Therefore, the assessment of Hb levels is critical for evaluating the health status of blood donors for several reasons, such as anaemia detection, donor eligibility, blood supply integrity, and health monitoring (54, 55). Appropriate Hb levels are essential to ensure the safety and well-being of blood donors during the donation process. Donors with Hb levels below specified thresholds may experience symptoms of hypoxia, fatigue, or dizziness due to reduced oxygen-carrying capacity (56).
Assessing Hb levels helps to determine the eligibility of individuals to safely donate blood, minimise the risk of adverse reactions, and ensure the quality of donated blood products. Hb levels are a reliable indicator of anaemia, a condition characterised by a reduced number of red blood cells or insufficient Hb content. Low Hb levels can indicate different types of anaemia, such as iron deficiency anaemia, vitamin B12 deficiency anaemia or haemolytic anaemia (57). Identifying anaemia in potential blood donors is essential to prevent adverse effects associated with blood donation, such as worsening of symptoms or complications (58).
The integrity of the blood supply and health surveillance play an important role in blood donation, as shown in publications (59, 60). Maintaining optimal Hb levels in blood donors contributes to the integrity and effectiveness of the blood supply chain. Donated blood with adequate Hb is essential to meet the oxygenation needs of recipients, particularly in transfusions for patients with anaemia, bleeding, or other medical conditions requiring blood replacement therapy (61). In our study, no changes in the Hb and Ht levels were observed, and the blood donors did not report any discomfort during medical interviews. Therefore, further analysis of iron levels was not warranted, as there was no evidence of iron deficiency or adverse effects associated with blood donation.
Monitoring Hb levels in donors helps maintain an adequate and reliable blood supply, supporting medical treatments and emergency interventions (62). Regular assessment of Hb levels in blood donors facilitates ongoing health monitoring and promotes early detection of underlying medical conditions or nutritional deficiencies. Changes in Hb levels over time may indicate changes in the donor’s health status, prompting further assessment, intervention, or referral for medical follow-up. By monitoring Hb levels, healthcare providers can identify potential health risks or abnormalities and take appropriate action to ensure the well-being of blood donors (63).
Secondly, our research investigated the effects of repeated blood donation on donor health and well-being, focusing on changes in red blood cell parameters. Furthermore, long-term blood donors exhibit a remarkable resilience of their hematopoietic system, characterized by robust stem cell activity and efficient erythropoietin production in response to blood loss. This adaptation ensures rapid recovery and minimal disruption to their overall health status following each donation. Moreover, multiple donors often display favourable lipid profiles and reduced risk factors for cardiovascular disease, attributed partially to the beneficial effects of blood donation on lipid metabolism and blood viscosity regulation (59, 60).
In our study, the determination of Ht levels in blood donors was shown to be essential for blood volume assessment, anaemia detection, blood quality assessment, and donor health screening. By monitoring Ht levels, healthcare professionals can ensure the safety of the blood donation process and promote the health and well-being of both donors and recipients. Ht measurement helps to estimate the volume of red blood cells in circulation, which is essential for maintaining adequate oxygen-carrying capacity and tissue perfusion (64). Monitoring Ht levels ensures that blood donors have sufficient circulating red blood cells to support physiological functions and meet the requirements of blood donation without compromising their own health. Our findings in the correlative analysis are confirmed by the summary correlations between Hb-Ht, as shown above, and Hb-RBC (r = 0.196, p = 0.000).
Some studies report that abnormally low Ht levels may indicate the presence of anaemia, a condition characterised by a reduced red blood cell count or Hb concentration (65, 66). Anaemia can be caused by a number of factors, including nutritional deficiencies, chronic disease, or underlying medical conditions. Identifying anaemia in blood donors is essential to prevent potential adverse effects associated with blood donation, such as worsening of symptoms or complications. Ht levels affect the viscosity and flow properties of blood, which in turn affect the quality and efficacy of donated blood products. Donors with extremely high or low Ht levels may be at increased risk of adverse reactions during or after blood donation, such as coagulopathy or hypervolemia. Assessment of Ht levels helps to ensure the safety and integrity of donated blood for transfusion purposes (67). It is important that regular monitoring of Ht levels is part of the comprehensive health screening process for blood donors. Changes in Ht levels over time may indicate changes in the donor’s health status and may prompt further evaluation, intervention, or referral for medical follow-up. By assessing Ht levels, healthcare providers can identify potential health risks or abnormalities in blood donors and take appropriate measures to ensure their well-being (66).
Thirdly, the analysis of data from multiple and long-term donors represents a unique subset within the donor population, characterised by their frequent and sustained commitment to blood donation over time. As such, they may have different characteristics in both their donation profiles and physiological parameters compared to occasional or first-time donors. Understanding these characteristics is critical for assessing the impact of repeated blood donation on donor health and well-being and for developing strategies to support the long-term health of these dedicated individuals (65). In the blood donation practice, the monitoring and interpretation of such blood parameters as MCHC, MCV, and MCH (Tab.4-6) are critical for assessing donor health and ensuring blood safety for patients (68). Gender differences may affect the reference values of these parameters (69). In a recent data analysis, the MCH value represents the average haemoglobin content per red blood cell and assists in the diagnosis of disease conditions, e.g. anaemia or haemoglobinopathies, through calculation based on total haemoglobin and red blood cell count (70).
MCHC (Mean Corpuscular Haemoglobin Concentration) reflects the concentration of Hb in red blood cells, with abnormal values potentially indicating such conditions as haemolytic anaemia or hypochromic anaemia (69). Therefore, the study of this parameter in our research showed statistical correlations in the following relationships: MCHC-MCH (r = 0.382, p = 0.000) and MCHC-MCV (r = -0.017, p = 0.035). The MCV (Mean Corpuscular Volume) parameter is the average size of red blood cells, calculated by dividing the total packed red blood cell volume by the total number of red blood cells. Therefore, changes in MCV levels serve as indicators of different types of anaemia, including microcytic, normocytic, or macrocytic anaemia, which is particularly important for donors (71-74). These studies have been published in a number of papers on haematology, demonstrating the relevance of monitoring these parameters not only in highly specialised groups, such as donors of different ages and genders (68, 69), considering the multiplicity of the donation process, as shown in our studies. The results of these tests are also a generally accepted indicator for prevention and health monitoring (70-72).
Fourthly, the results of our study show that a notable aspect of multiple and long-term donors is the donation frequency. Unlike occasional or first-time donors, who may donate sporadically, these individuals tend to donate regularly and often more frequently. As a result, they may have higher cumulative donation volumes and shorter intervals between donations. This frequent exposure to the blood donation process may affect several physiological parameters, such as Hb levels, iron stores, and erythropoietin production (73, 74).
Fifthly, based on our findings, we propose strategies to support the long-term health of multiple and long-term blood donors, including regular monitoring of their health, individualised advice on iron supplementation and dietary recommendations, and collaboration with healthcare providers to address specific health concerns. The multiple regression analysis performed on the dependent variables, such as Hb, Ht, RBC count, MCH, MCHC, and MCV, yielded significant results, as our chosen statistical model explained a substantial amount of the variance in the dependent variables. Importantly, the relationships between the predictor variables collectively contribute to their prediction. As shown in this study, individual predictors (age, donor gender, and frequency of donation) have varying degrees of influence on the dependent variables, with some showing strong positive or negative associations. We can claim that the overall fit of the statistical model presented in this study in relation to donors is satisfactory, as evidenced by the goodness of fit statistics. However, further analysis is recommended to explore potential multicollinearity and outliers that may affect the reliability of the regression results. Overall, the regression analysis performed in this study provides valuable information on the relationship between the dependent variables representing the morphological parameters of the red blood cells and the three predictors, providing a basis for further research and decision making in donor practice, which is a valuable material.
In addition, long-term blood donors may have unique immunological profiles characterised by increased immune responsiveness and antibody production. Regular exposure to foreign antigens present in donated blood stimulates the donor’s immune system, leading to the development of a diverse antibody repertoire and potentially conferring protective immunity against certain infections (75-78).
Important aspects of the influence of donor gender on disease occurrence have been addressed in a number of studies using the example of the majority of cases of transfusion-related acute lung injury (TRALI) associated with female blood donors. In an international multicentre case study, the authors (56) investigated the relationship between female donors and the occurrence of TRALI by recruiting patients with a clinical diagnosis, irrespective of serology or donor sex, who received blood transfusions exclusively from male or female donors. These results suggest that plasma from female donors is associated with an increased risk of TRALI, in contrast to red cells from female donors. However, in a secondary analysis of two case-control studies (79), other authors concluded that donor age, donor sex, and donor blood group were not associated with TRALI in two cohorts of TRALI patients (80).
Our research investigates the effects of repeated blood donation on the health and well-being of donors, focusing on changes in red blood cell parameters, which will help inform future analyses of iron metabolism markers and cardiovascular function. Overall, the comprehensive understanding of the biological adaptations and physiological responses observed in multiple and long-term blood donors sheds light on their remarkable capacity for sustained donation and underlines the importance of recognising their invaluable contribution to the blood supply.
Conclusion
In conclusion, multiple and long-term blood donors are essential pillars of the blood donation system and contribute significantly to the availability and sustainability of the blood supply. The aim of our study was to analyse the levels of haemoglobin, haematocrit, erythrocyte count, MCV, MCH, and MCHC in 12 groups of first-time donors and experienced donors of both sexes at the John Paul II Regional Blood Donation and Treatment Centre in Słupsk, northern Poland. The donors were divided into three age groups (18-30 years, 31-45 years, and 46-65 years). The multivariate analysis of these three main factors showed that the variation in haemoglobin (Hb) levels accounted for 46% of the explained dependence in this statistical model. In particular, approximately half of the variability in the multivariate statistical analysis was attributed to the role of Hb and haematocrit (Ht), respectively. In addition, the β-coefficient values for Hb and Ht were statistically higher in relation to donor gender and donor type (one-time versus repeat). A comprehensive analysis of the whole statistical model of the biomarkers of metabolic processes revealed the following hierarchy: Hb > Ht > MCHC > MCV > RBC > MCH. Our statistical model showed a good overall fit, and its credibility was supported by various statistics, including the coefficient of determination (R²), the F-test statistic, and other metrics.
Recognising their contribution and understanding their unique characteristics is critical for ensuring the continued success of blood donation programmes and the well-being of both donors and recipients. Our research represents a pioneering effort to explore the unique characteristics of multiple and long-term donors and their impact on donor health and well-being. By shedding light on these important issues, we aim to improve our understanding of blood donation practices and contribute to the development of effective strategies to support the long-term health of committed blood donors.
Acknowledgements
The present study was financially supported by the Pomeranian University in Słupsk. The authors would like to thank the John Paul II Regional Blood Donation and Treatment Centre in Słupsk and Pomeranian University in Słupsk for supporting this research.
Ethical approval
The experiments were conducted by the Guidelines of the European Union Council and the current laws in Poland. The study was conducted with the statement on bioethical approval of the Bioethics Committee of Gdansk (KB 41/23). All studies involving human blood were approved by the institutional review board of the Bioethical Commission at Gdańsk Medical University (No KB-41/23, 9.10.2023).
Authors’ contributions
Natalia Kurhaluk, ORCID: https://orcid.org/0000-0002-4669-1092;
Małgorzata Gradziuk, ORCID: https://orcid.org/0009-0008-7064-5214
Piotr Kamiński, ORCID: https://orcid.org/0000-0003-1978-6018;
Halina Tkaczenko, ORCID: https://orcid.org/0000-0003-3951-9005
The authors contributed to the following aspects of the study: Conceptualization: NK, HT, PK, MG; Data curation: HT, NK; Formal analysis: HT, NK; Investigation: HT, NK, MG; Methodology: HT, NK, PK, MG; Supervision: NK, HT; Writing – original draft: NK, PK, HT; Writing – revision and editing: HT, NK, PK, MG.
Funding
The present study was financially supported by the Pomeranian University in Słupsk.
Disclosure Statement
The authors have no competing interests to declare.
References
| 1 | WHO: Blood safety and availability. World Health Organization. 2020 https://www.who.int/news-room/fact-sheets/detail/blood-safety-and-availability.
|
| 2 | Glynn SA, Kleinman SH, Schreiber GB, Busch MP, Wright DJ, Smith JW, Nass CC, Williams AE: Trends in incidence and prevalence of major transfusion-transmissible viral infections in US blood donors, 1991 to 1996 Retrovirus Epidemiology Donor Study (REDS). JAMA 2000;284:229-235.
https://doi.org/10.1001/jama.284.2.229 |
| 3 | Morse EE, Cable R, Pisciotto P, Kakaiya R, Kiraly T: Evaluation of iron status in women identified by copper sulfate screening as ineligible to donate blood. Transfusion 1987;27:238-241.
https://doi.org/10.1046/j.1537-2995.1987.27387235628.x |
| 4 | Cable RG, Morse EE, Keltonic J, Kakaiya R, Kiraly T: Iron supplementation in female blood donors deferred by copper sulfate screening. Transfusion 1988;28:422-426.
https://doi.org/10.1046/j.1537-2995.1988.28588337328.x |
| 5 | Kiss JE: Laboratory and genetic assessment of iron deficiency in blood donors. Clin Lab Med. 2015;35:73-91.
https://doi.org/10.1016/j.cll.2014.10.011 |
| 6 | Reddy KV, Shastry S, Raturi M, Baliga BP: Impact of Regular Whole-Blood Donation on Body Iron Stores. Transfus Med Hemother 2020;47:75-79.
https://doi.org/10.1159/000499768 |
| 7 | Sayers M: Donor iron nutrition: Which precaution prevails?. Transfusion 2021;61:313-317.
https://doi.org/10.1111/trf.16158 |
| 8 | Spencer BR, White JL, Patel EU, Goel R, Bloch EM, Tobian AA: Eligibility Considerations for Female Whole Blood Donors: Hemoglobin Levels and Iron Status in a Nationally Representative Population. Transfus Med Rev 2023;37:27-35.
https://doi.org/10.1016/j.tmrv.2022.11.001 |
| 9 | Firth J, Gangwisch JE, Borisini A, Wootton RE, Mayer EA: Food and mood: how do diet and nutrition affect mental wellbeing? BMJ 2020;369:m2382.
https://doi.org/10.1136/bmj.m2382 |
| 10 | Cena H, Calder PC. Defining a Healthy Diet: Evidence for The Role of Contemporary Dietary Patterns in Health and Disease. Nutrients. 2020;12:334.
https://doi.org/10.3390/nu12020334 |
| 11 | Feng W, Yun W, Le W, Zhi-Guo X, Hai-Ying Y, Shu-Fang W, Zhen-Yan W, Yi-Zhu C, Quan S, Jing-Xian F: The influence of demographic and lifestyle factors on blood donation delay among student population: a retrospective study. Front Public Health 2023;11:1297472.
https://doi.org/10.3389/fpubh.2023.1297472 |
| 12 | Lobier M, Castrén J, Niittymäki P, Palokangas E, Partanen J, Arvas M: The effect of donation activity dwarfs the effect of lifestyle, diet and targeted iron supplementation on blood donor iron stores. PLoS One 2019;14:e0220862.
https://doi.org/10.1371/journal.pone.0220862 |
| 13 | Mousavi SA, Hermundstad B, Saether PC, Nybruket MJ, Knutsen TR, Llohn AH: Health Behavior and Lifestyle Trends among Platelet Donors: Results from a Questionnaire-Based Survey in Norway. Biomed Res Int 2021;2021:8891885.
https://doi.org/10.1155/2021/8891885 |
| 14 | Schlumpf KS, Glynn SA, Schreiber GB, Wright DJ, Randolph Steele W, Tu Y, Hermansen S, Higgins MJ, Garratty G, Murphy EL: National Heart, Lung, and Blood Institute Retrovirus Epidemiology Donor Study. Factors influencing donor return. Transfusion 2008;48:264-272.
https://doi.org/10.1111/j.1537-2995.2007.01519.x |
| 15 | Vassallo RR, Bravo MD, Kamel H: Ferritin testing to characterize and address iron deficiency in young donors. Transfusion 2018;58:2861-2867.
https://doi.org/10.1111/trf.14921 |
| 16 | Vassallo R, Kamel H, Goel R, Al-Riyami AZ, Al Muharrmi Z, Jacquot C, Ramirez-Arcos S, Khandelwal A, Goldman M, Hands K, McLintock L, Mitchell H, Wendel S, Scuracchio P, Fachini R, Pettersson SM, Bengtsson J, Brailsford SR, Tossell J, Amorim L, Lopes ME, Pêcego M, Germain M, Renaud C, Morley SL, So R, Townsend M, Hopkins C, Harritshoej LH, Erikstrup C, Gosbell IB, Levin MH, Dennington PM, Dunbar N: International Forum on Management of Blood Donors with Culture-Positive Platelet Donations: Summary. Vox Sang 2023;118:997-1003.
https://doi.org/10.1111/vox.13519 |
| 17 | France JL, France CR, Himawan LK: A path analysis of intention to redonate among experienced blood donors: an extension of the theory of planned behavior. Transfusion. 2007;47:1006-1013.
https://doi.org/10.1111/j.1537-2995.2007.01236.x |
| 18 | Veldhuizen IJ, Doggen CJ, Atsma F, De Kort WL: Donor profiles: demographic factors and their influence on the donor career. Vox Sang 2009;97:129-138.
https://doi.org/10.1111/j.1423-0410.2009.01201.x |
| 19 | Rosiek A, Nieradkiewicz A, Lachert E, Antoniewicz-Papis J, Lasocka J, Łetowska M: Blood transfusion service in Poland in 2021 Journal of Transfusion Medicine 2022;15:273-295.
https://doi.org/10.5603/JTM.2022.0018 |
| 20 | Masser BM, Bednall TC, White KM, Terry D: Predicting the retention of first-time donors using an extended Theory of Planned Behavior. Transfusion 2012;52:1303-1310.
https://doi.org/10.1111/j.1537-2995.2011.03479.x |
| 21 | Steele WR, Schreiber GB, Guiltinan A, Nass C, Glynn SA, Wright DJ, Kessler D, Schlumpf KS, Tu Y, Smith JW, Garratty G: Retrovirus Epidemiology Donor Study. role of altruistic behavior, empathetic concern, and social responsibility motivation in blood donation behavior. Transfusion 2008;48:43-54.
https://doi.org/10.1111/j.1537-2995.2007.01481.x |
| 22 | Bednall TC, Bove LL, Cheetham A, Murray AL: A systematic review and meta-analysis of antecedents of blood donation behavior and intentions. Soc Sci Med 2013;96:86-94 .
https://doi.org/10.1016/j.socscimed.2013.07.022 |
| 23 | Godin G, Sheeran P, Conner M, Germain M: Asking questions changes behavior: mere measurement effects on frequency of blood donation. Health Psychol 2008;27:179-184.
https://doi.org/10.1037/0278-6133.27.2.179 |
| 24 | Bednall TC, Bove LL: Donating blood: a meta-analytic review of self-reported motivators and deterrents. Transfus Med Rev 2011;25:317-34.
https://doi.org/10.1016/j.tmrv.2011.04.005 |
| 25 | Bagot KL, Murray AL, Masser BM: How Can We Improve Retention of the First-Time Donor? A Systematic Review of the Current Evidence. Transfus Med Rev 2016;30:81-91.
https://doi.org/10.1016/j.tmrv.2016.02.002 |
| 26 | Piersma TW, Bekkers R, Klinkenberg EF, De Kort WLAM, Merz EM: Individual, contextual and network characteristics of blood donors and non-donors: a systematic review of recent literature. Blood Transfus 2017;15:382-397.
|
| 27 | Siekierska B, Tomaszek L, Kurleto P, Turkanik E, Mędrzycka-Dąbrowska W: Blood donation practice and its associated factors among Polish population: secondary data analysis. Front Public Health. 2023;11:1251828.
https://doi.org/10.3389/fpubh.2023.1251828 |
| 28 | Buratti P, Gammella E, Rybinska I, Cairo G, Recalcati S: Recent Advances in Iron Metabolism: Relevance for Health, Exercise, and Performance. Med Sci Sports Exerc 2015;47:1596-1604.
https://doi.org/10.1249/MSS.0000000000000593 |
| 29 | Dixon SJ, Stockwell BR: The role of iron and reactive oxygen species in cell death. Nat Chem Biol 2014;10:9-17. DOI:10.1038/nchembio.1416.
https://doi.org/10.1038/nchembio.1416 |
| 30 | Moll R, Davis B: Iron, vitamin B12 and folate. Medicine 2017;45:198-203.
https://doi.org/10.1016/j.mpmed.2017.01.007 |
| 31 | Zappacosta B, Persichilli S, Iacoviello L: Folate, vitamin B12 and homocysteine status in an Italian blood donor population. Nutr Metab Cardiovasc Dis 2013;23:473-480.
https://doi.org/10.1016/j.numecd.2011.10.001 |
| 32 | Popkin BM, D'Anci KE, Rosenberg IH: Water, hydration, and health. Nutr Rev 2010;68:439-458.
https://doi.org/10.1111/j.1753-4887.2010.00304.x |
| 33 | Rushton DH, Barth JH: What is the evidence for gender differences in ferritin and haemoglobin?. Crit Rev Oncol Hematol 2010;73:1-9.
https://doi.org/10.1016/j.critrevonc.2009.03.010 |
| 34 | Chen WL: Body Donation Registration in Taiwan: Reasons and Associated Psychological Factors. Healthcare (Basel). 2023;11:969.
https://doi.org/10.3390/healthcare11070969 |
| 35 | Spencer BR, Mast AE: Iron status of blood donors. Curr Opin Hematol 2022;29:310-316.
https://doi.org/10.1097/MOH.0000000000000733 |
| 36 | Spencer B: Blood donor iron status: are we bleeding them dry? Curr Opin Hematol 2013;20:533-539.
https://doi.org/10.1097/MOH.0b013e32836589f2 |
| 37 | Spencer BR, Haynes JM, Notari EP 4th, Stramer SL: Prevalence, risk factors, and ferritin testing to mitigate iron depletion in male plateletpheresis donors. Transfusion 2020;60:759-768.
https://doi.org/10.1111/trf.15729 |
| 38 | Vassallo R, Kamel H, Goel R, Al-Riyami AZ, Al-Muharrmi Z, Jacquot C, Ramirez-Arcos S, Khandelwal A, Goldman M, Hands K, McLintock L, Mitchell H, Wendel S, Scuracchio P, Fachini R, Pettersson SM, Bengtsson J, Brailsford SR, Tossell J, Amorim L, Lopes ME, Pêcego M, Germain M, Renaud C, Morley SL, So R, Townsend M, Hopkins C, Harritshoej LH, Erikstrup C, Gosbell IB, Levin MH, Dennington PM, Dunbar N: International Forum on Management of Blood Donors with Culture-Positive Platelet Donations: Responses. Vox Sang. 2023;118:1004-1023.
https://doi.org/10.1111/vox.13520 |
| 39 | Schreiber GB, Busch MP, Kleinman SH, Korelitz JJ. The risk of transfusion-transmitted viral infections. The Retrovirus Epidemiology Donor Study. N Engl J Med 1996;334:1685-1690.
https://doi.org/10.1056/NEJM199606273342601 |
| 40 | Cable RG, Glynn SA, Kiss JE, Mast AE, Steele WR, Murphy EL, Wright DJ, Sacher RA, Gottschall JL, Vij V, Simon TL: NHLBI Retrovirus Epidemiology Donor Study-II. Iron deficiency in blood donors: analysis of enrollment data from the REDS-II Donor Iron Status Evaluation (RISE) study. Transfusion 2011;51:511-522.
https://doi.org/10.1111/j.1537-2995.2010.02865.x |
| 41 | Torreiter PP, Drexler-Helmberg C, Schimetta W, Krakowitzky P, Helmberg W, Schlenke P: Pilot Study to Gain First Indications for the Impact of a 3-Month's Oral Intake of a Sucrosomial Iron Supplement on Hemoglobin in Iron-Deficient Blood Donors. Transfus Med Hemother 2022;50:286-293.
https://doi.org/10.1159/000527577 |
| 42 | Peffer K, Verbeek AL, Swinkels DW, Geurts-Moespot AJ, den Heijer M, Atsma F: Donation intensity and metabolic syndrome in active whole-blood donors. Vox Sang 2015;109:25-34.
https://doi.org/10.1111/vox.12258 |
| 43 | Trouern-Trend JJ, Cable RG, Badon SJ, Newman BH, Popovsky MA: A case-controlled multicenter study of vasovagal reactions in blood donors: influence of sex, age, donation status, weight, blood pressure, and pulse. Transfusion 1999;39:316-320.
https://doi.org/10.1046/j.1537-2995.1999.39399219291.x |
| 44 | Philip J, Sarkar RS, Jain N: A single-centre study of vasovagal reaction in blood donors: Influence of age, sex, donation status, weight, total blood volume and volume of blood collected. Asian J Transfus Sci. 2014;8:43-46.
https://doi.org/10.4103/0973-6247.126690 |
| 45 | Rosiek A, Nieradkiewicz A, Lachert E., Antoniewicz-Papis J, Lasocka J, Łętowska M: Blood transfusion service in Poland in 2022 J Transf Med 2023;16:167-188.
https://doi.org/10.5603/jtm.99300 |
| 46 | Journal of Laws of the Republic of Poland, Warsaw, June 20, 2022, Item 1279. Regulation of the Minister of Health of September 11, 2017, on the conditions for collecting blood from blood donor candidates and blood donors, Journal of Laws 2017, item 1741.
|
| 47 | Kiss JE, Vassallo RR: How do we manage iron deficiency after blood donation? Br J Haematol 2018;181(5):590-603 DOI: 10.1111/bjh.15136.
https://doi.org/10.1111/bjh.15136 |
| 48 | Hadjesfandiari N, Khorshidfar M, Devine DV: Current Understanding of the Relationship between Blood Donor Variability and Blood Component Quality. Int J Mol Sci 2021;22:3943.
https://doi.org/10.3390/ijms22083943 |
| 49 | Kaptoge S, Di Angelantonio E, Moore C, Walker M, Armitage J, Ouwehand WH, Roberts DJ, Danesh J, Thompson SG: INTERVAL Trial Group. Longer-term efficiency and safety of increasing the frequency of whole blood donation (INTERVAL): extension study of a randomised trial of 20 757 blood donors. Lancet Haematol 2019;6:510-520
https://doi.org/10.1016/S2352-3026(19)30106-1 |
| 50 | Stanisz A: An affordable statistics course using STATISTICA PL on examples from medicine. Volume 2 Liniear and non-linear models - in Polish. StatSoft, Kraków, 2007.
|
| 51 | Fabijańska-Mitek, J., Mariańska, B., Windyga, J: Laboratory tests in hematology. Textbook for medical students. 2006. PZWL Wydawnictwo Lekarskie, Warszawa.
|
| 52 | De Clippel D, Van Heddegem L, Vandewalle G, Vandekerckhove P, Compernolle V: Hemoglobin screening in blood donors: a prospective study assessing the value of an invasive and a noninvasive point-of-care device for donor safety. Transfusion 2017;57:938-945.
https://doi.org/10.1111/trf.13987 |
| 53 | Brandow AM, Liem RI: Advances in the diagnosis and treatment of sickle cell disease. J Hematol Oncol 2022;15:20.
https://doi.org/10.1186/s13045-022-01237-z |
| 54 | Gaddam M, Prakash P, Devegowda D, Kumar R: Analysis of JAK2V617F Tyrosine Kinase Mutation in Blood Donors with Erythrocytosis - A Pilot Study in a Tertiary Care Teaching Hospital of South India. J Blood Med 2022;13:439-446.
https://doi.org/10.2147/JBM.S370687 |
| 55 | Mendrone A Jr, Sabino EC, Sampaio L, Neto CA, Schreiber GB, Chamone Dde A, Dorlhiac-Llacer PE: Anemia screening in potential female blood donors: comparison of two different quantitative methods. Transfusion. 2009;49:662-668.
https://doi.org/10.1111/j.1537-2995.2008.02023.x |
| 56 | Zervou EK, Ziciadis K, Karabini F, Xanthi E, Chrisostomou E, Tzolou A: Vasovagal reactions in blood donors during or immediately after blood donation. Transfus Med 2005;15:389-394.
https://doi.org/10.1111/j.1365-3148.2005.00600.x |
| 57 | Baart AM, de Kort WL, Moons KG, Atsma F, Vergouwe Y: Zinc protoporphyrin levels have added value in the prediction of low hemoglobin deferral in whole blood donors. Transfusion 2013;53:1661-1669.
https://doi.org/10.1111/j.1537-2995.2012.03957.x |
| 58 | Lotfi R, Wernet D, Starke U, Northoff H, Cassens U: A noninvasive strategy for screening prospective blood donors for anemia. Transfusion 2005;45:1585-1592.
https://doi.org/10.1111/j.1537-2995.2005.00574.x |
| 59 | Eder A: Evidence-based selection criteria to protect blood donors. J Clin Apher. 2010;25:331-337.
https://doi.org/10.1002/jca.20257 |
| 60 | Eder A, Goldman M, Rossmann S, Waxman D, Bianco C: Selection criteria to protect the blood donor in North America and Europe: past (dogma), present (evidence), and future (hemovigilance). Transfus Med Rev. 2009;23:205-220.
https://doi.org/10.1016/j.tmrv.2009.03.003 |
| 61 | Luban NL: Transfusion safety: Where are we today? Ann N Y Acad Sci 2005;1054:325-341.
https://doi.org/10.1196/annals.1345.040 |
| 62 | Rigas AS, Pedersen OB, Magnussen K, Erikstrup C, Ullum H: Iron deficiency among blood donors: experience from the Danish Blood Donor Study and from the Copenhagen ferritin monitoring scheme. Transfus Med 2019;29:23-27.
https://doi.org/10.1111/tme.12477 |
| 63 | Ziemann M, Steppat D, Brockmann C, Washington G, Kirchner H, Schlenke P: Selection of whole-blood donors for hemoglobin testing by use of historical hemoglobin values. Transfusion 2006;46:2176-2183.
https://doi.org/10.1111/j.1537-2995.2006.01049.x |
| 64 | Tagariello G, Di Gaetano R, Sartori R, Zanotto D, Belvini D, Radossi P, Risato R, Roveroni G, Salviato R, Tassinari C, Toffano N: The JAK2(V617F) tyrosine kinase mutation in blood donors with upper-limit haematocrit levels. Blood Transfus 2009;7:111-116.
|
| 65 | Young S, Fink A, Geiger S, Marbella A, Mast AE, Schellhase KG: Community blood donors' knowledge of anemia and design of a literacy-appropriate educational intervention. Transfusion 2010;50:75-79.
https://doi.org/10.1111/j.1537-2995.2009.02358.x |
| 66 | Delaney M, Schellhase KG, Young S, Geiger S, Fink A, Mast AE: Blood center practice and education for blood donors with anemia. Transfusion 2011;51:929-936.
https://doi.org/10.1111/j.1537-2995.2010.02919.x |
| 67 | Hirani R, Mondy P: Review of full blood count reference interval using a large cohort of first-time plasmapheresis blood donors. Pathology 2021;53:498-502.
https://doi.org/10.1016/j.pathol.2020.08.013 |
| 68 | Merz EM, Zijlstra BJH, de Kort WLAM: Blood donor show behaviour after an invitation to donate: The influence of collection site factors. Vox Sang 2017 Oct;112:628-637.
https://doi.org/10.1111/vox.12562 |
| 69 | Zhong WJ, Zhang QF, Huang CY, Chen YC, Zhou YP, Chen JY, Zeng J: [Relationship between Iron Metabolic Parameters and Platelet Counts in Blood Donors]. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2023;31:1481-1485.
|
| 70 | Hipgrave DB, Laksmono LH, Koemarasakti GM, Nandy R, Setiawan B, Hermawan L, Marbun D: District team problem solving as an approach to district health programme planning: a review, and survey of its status in selected districts in Indonesia. Health Policy Plan 2018;33:555-563.
https://doi.org/10.1093/heapol/czy007 |
| 71 | Gillespie TW, Hillyer CD: Blood donors and factors impacting the blood donation decision. Transfus Med Rev 2002;16:115-130.
https://doi.org/10.1053/tmrv.2002.31461 |
| 72 | Brugnara C, Chambers LA, Malynn E, Goldberg MA, Kruskall MS: Red blood cell regeneration induced by subcutaneous recombinant erythropoietin: iron-deficient erythropoiesis in iron-replete subjects. Blood 1993;81:956-964.
https://doi.org/10.1182/blood.V81.4.956.bloodjournal814956 |
| 73 | Jacobs P, Wood L, Bird AR: Erythrocytes: Better Tolerance of Iron Polymaltose Complex Compared with Ferrous Sulphate in the Treatment of Anaemia. Hematology 2000;5:77-83.
https://doi.org/10.1080/10245332.2000.11746490 |
| 74 | Vuk T, Bingulac-Popović J, Očić T, Mayer LJ, Milošević M, Jukić I: Combined cell index in assessing blood donor iron stores. Transfus Med 2017;27:16-24.
https://doi.org/10.1111/tme.12370 |
| 75 | Schreiber GB, Brinser R, Rosa-Bray M, Yu ZF, Simon T: Frequent source plasma donors are not at risk of iron depletion: the Ferritin Levels in Plasma Donor (FLIPD) study. Transfusion 2018;58:951-959.
https://doi.org/10.1111/trf.14489 |
| 76 | Shanwell A, Kristiansson M, Remberger M, Ringdén O: Generation of cytokines in red cell concentrates during storage is prevented by prestorage white cell reduction. Transfusion 1997;37:678-684.
https://doi.org/10.1046/j.1537-2995.1997.37797369441.x |
| 77 | Edgren G, Hjalgrim H, Reilly M, Tran TN, Rostgaard K, Shanwell A, Titlestad K, Adami J, Wikman A, Jersild C, Gridley G, Wideroff L, Nyrén O, Melbye M: Risk of cancer after blood transfusion from donors with subclinical cancer: a retrospective cohort study. Lancet 2007;369:1724-1730 .
https://doi.org/10.1016/S0140-6736(07)60779-X |
| 78 | Saqlain N, Mazher N, Arshad S, Sajjal M: Effect of donor and red blood cells concentrate characteristics on recipient hemoglobin increment following red blood cells transfusion in pediatric patients. Pak J Med Sci 2022;38:1420-1425.
https://doi.org/10.12669/pjms.38.6.5739 |
| 79 | Middelburg RA, Van Stein D, Zupanska B, Uhrynowska M, Gajic O, Muñiz-Diaz E, Galvez NN, Silliman CC, Krusius T, Wallis JP, Vandenbroucke JP, Briët E, Van Der Bom JG: Female donors and transfusion-related acute lung injury: A case-referent study from the International TRALI Unisex Research Group. Transfusion 2010;50:2447-2454.
https://doi.org/10.1111/j.1537-2995.2010.02715.x |
| 80 | Peters AL, van de Weerdt EK, Prinsze F, de Korte D, Juffermans NP, Vlaar APJ: Donor characteristics do not influence transfusion-related acute lung injury incidence in a secondary analysis of two case-control studies. Transfus Clin Biol 2019;26:10-17.
https://doi.org/10.1016/j.tracli.2018.05.003 |